What is your diagnosis?
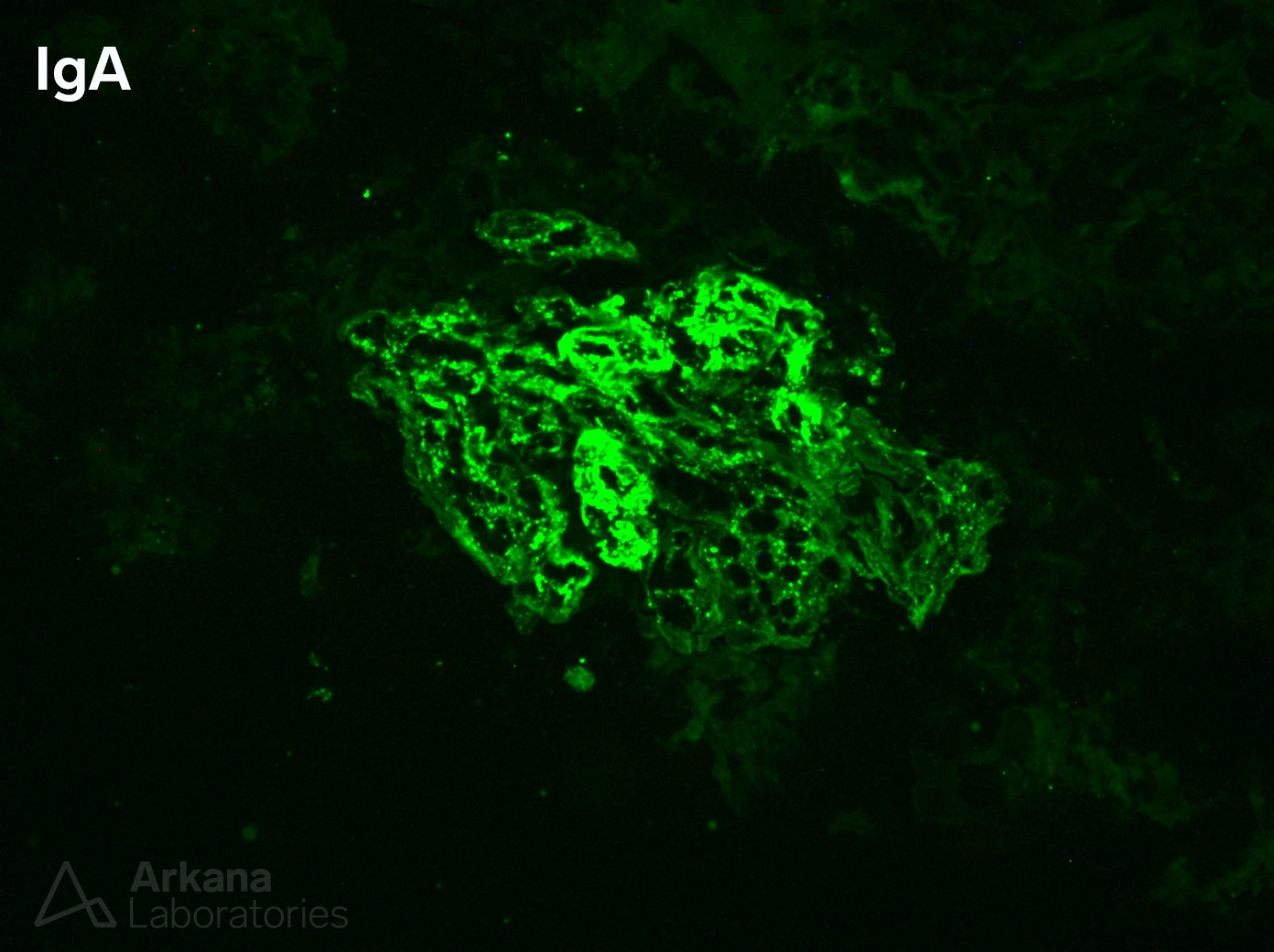
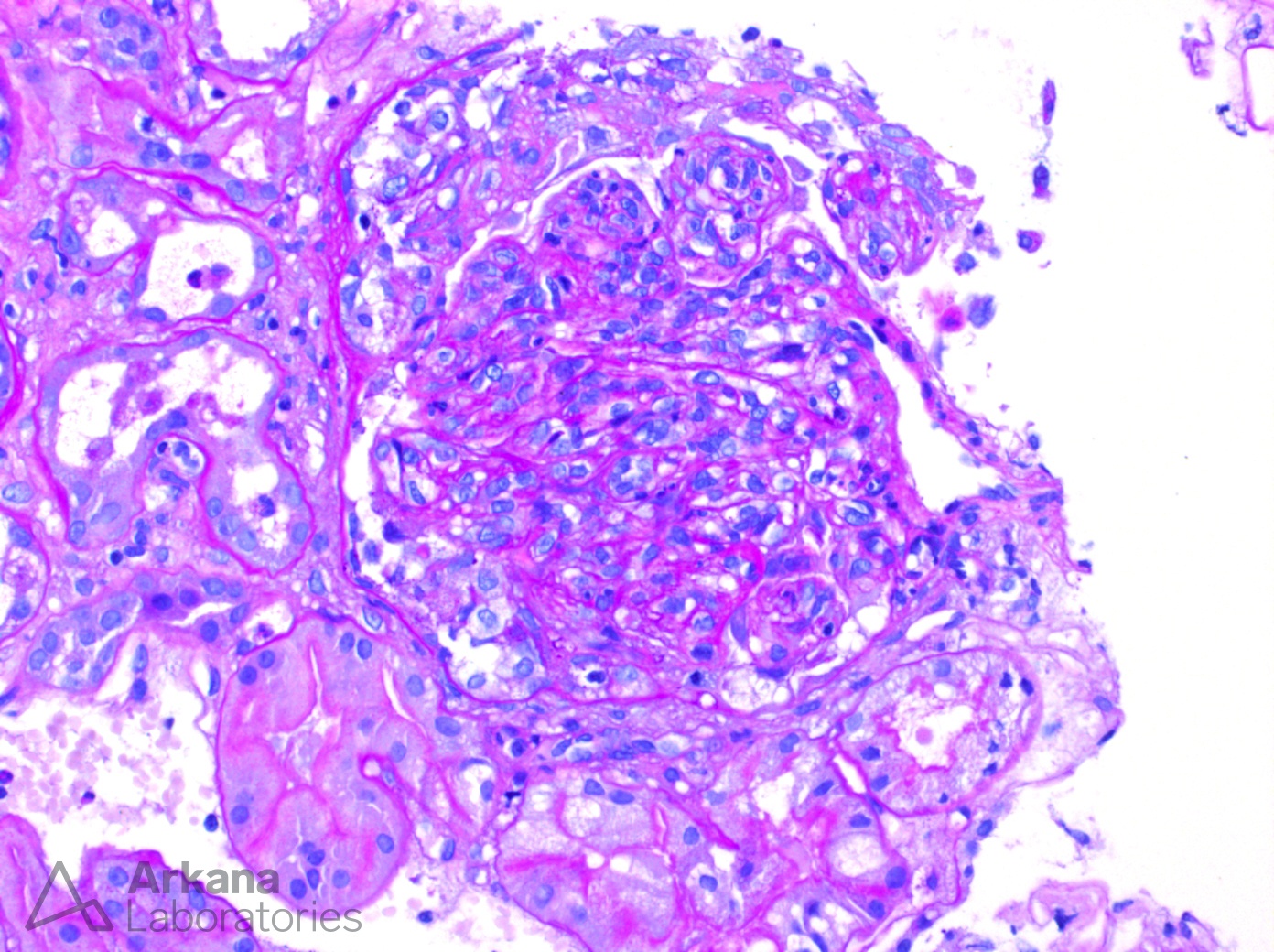
The images show a necrotizing, crescentic, and endocapillary proliferative glomerulonephritis with IgA deposition and is most suggestive of an IgA dominant infection-associated glomerulonephritis. This is a disease that is most often seen in diabetic patients with underlying Staphylococcal sp. infections. Additional, helpful biopsy clues include C3 staining that is more intense than IgA, subepithelial ‘hump-shaped’ deposits, and intracapillary neutrophils although these are not always seen. These cases can be difficult to distinguish from proliferative IgA nephropathy and can sometimes even mimic the clinical presentation of Henoch Schönlein purpura in adult patients. Treatment of this lesion is typically directed at resolving the underlying infection, however some nephrologists will also choose immunosuppression (in this case a course of corticosteroids was prescribed) when the proliferative glomerular changes are diffuse and severe. Unfortunately, no randomized controlled trials exist to evaluate the efficacy of immunosuppression in IgA dominant infection-associated glomerulonephritis and this entity is not addressed in the KDIGO GN guidelines. It should be noted that even with successful treatment of the underlying infection and resolution of the IGAGN that approximately 80% of patients with this entity and concurrent diabetic glomerulopathy will progress to end stage renal disease within two years.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.