What is your diagnosis?
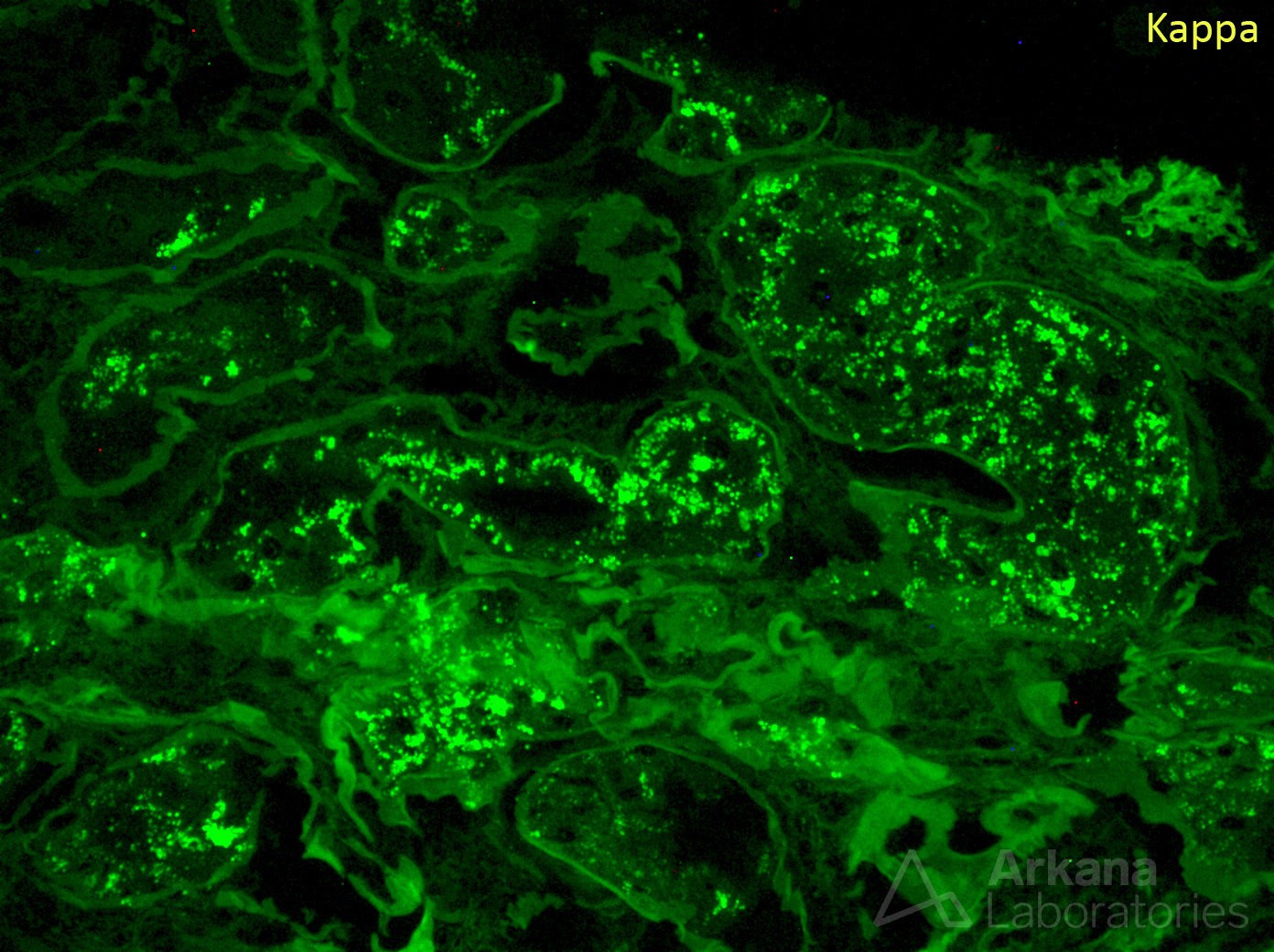
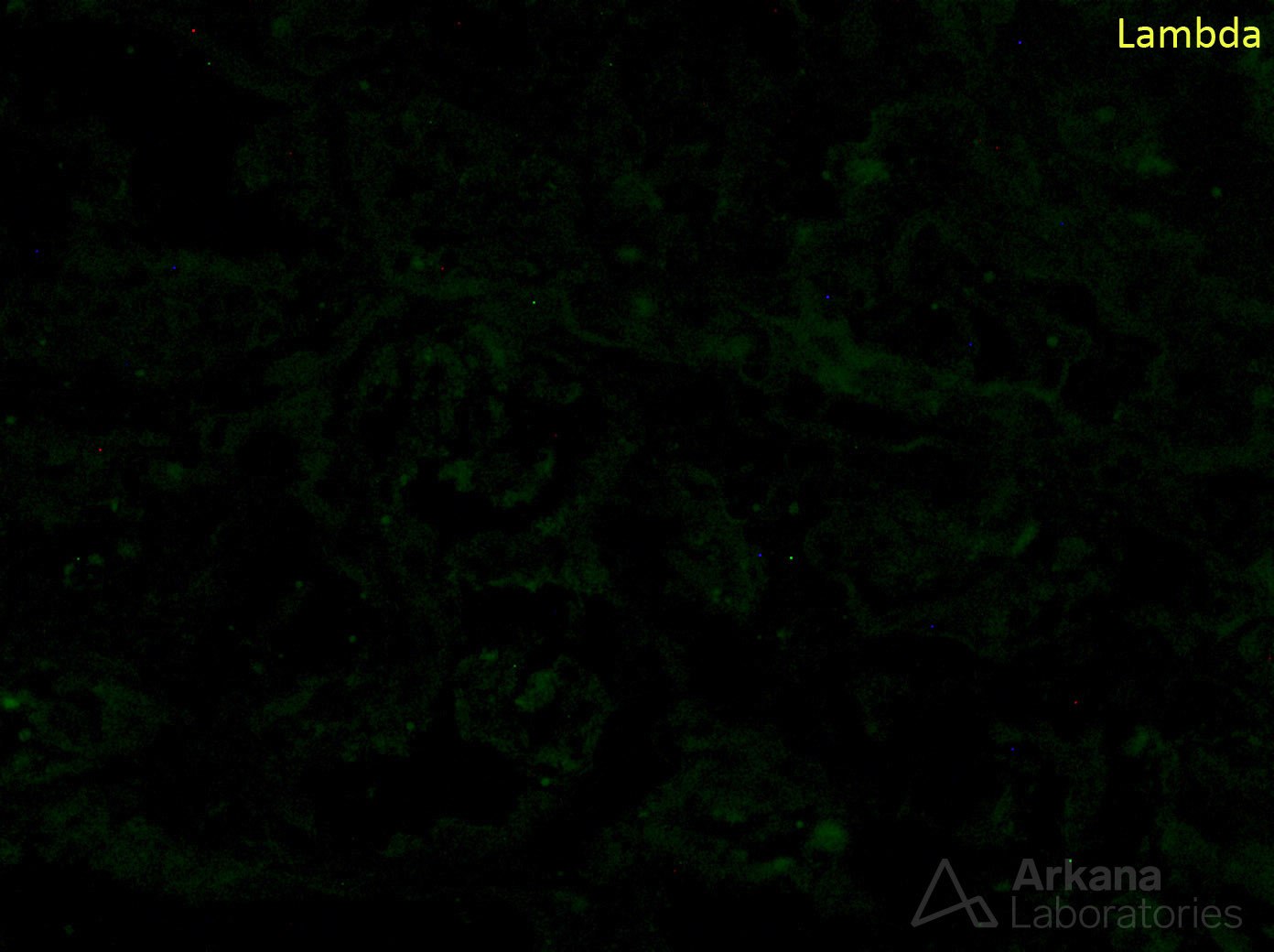
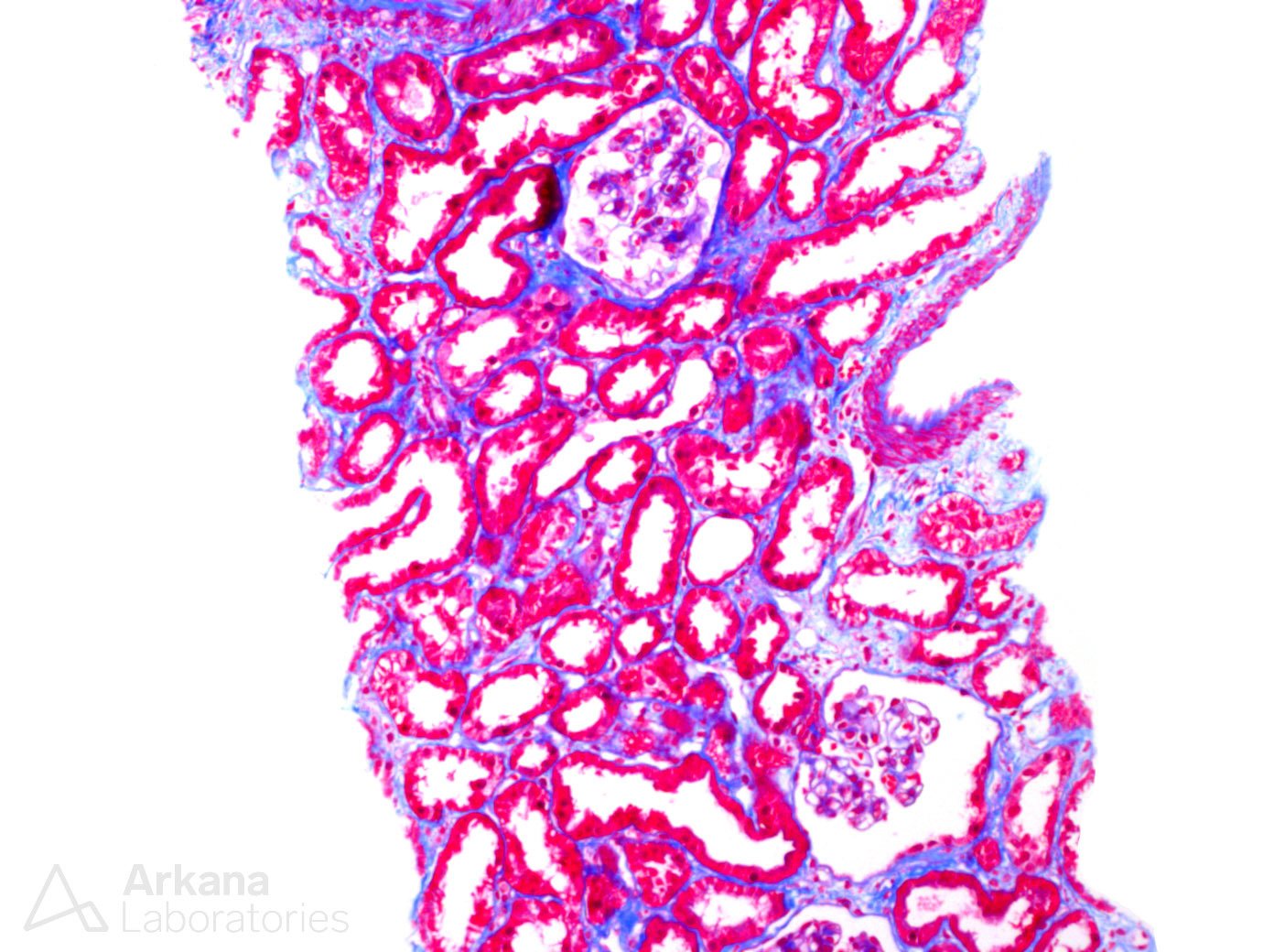
The images show proximal tubules with kappa light chain restriction within the protein resorption droplets, which do not appear to have a crystalline morphology. This finding raises a differential diagnosis of non-crystalline light chain proximal tubulopathy vs. non-specific physiologic trafficking in the setting of MGUS (the patient had a documented kappa light chain MGUS and very high kappa free light chains). Unfortunately, definitive diagnosis of whether this finding represents a monoclonal gammopathy of renal significance can be impossible to achieve and differentiation often is made on a combination of clinical and morphologic factors. Different renal pathologists handle this lesion differently and there is no consensus on how this lesion should be handled clinically. However, a few good rules of thumb can be applied here. First, is there good evidence of acute tubular injury within the biopsy? If not then it is difficult to say these findings are causing end organ damage. Next, is there any other clinically identifiable etiology for the patient’s acute tubular injury? While acute tubular injury often occurs in the absence of a known clinical etiology, this is still an important question to ask as often the patient has other reasons to have acute tubular injury. And, lastly, as non-crystalline proximal tubulopathy is typically a persistent, slowly progressive entity, it is often advisable ‘wait and watch’ to make sure the patient does not spontaneously resolve their acute kidney injury/proteinuria with supportive care in a typical timeframe.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.