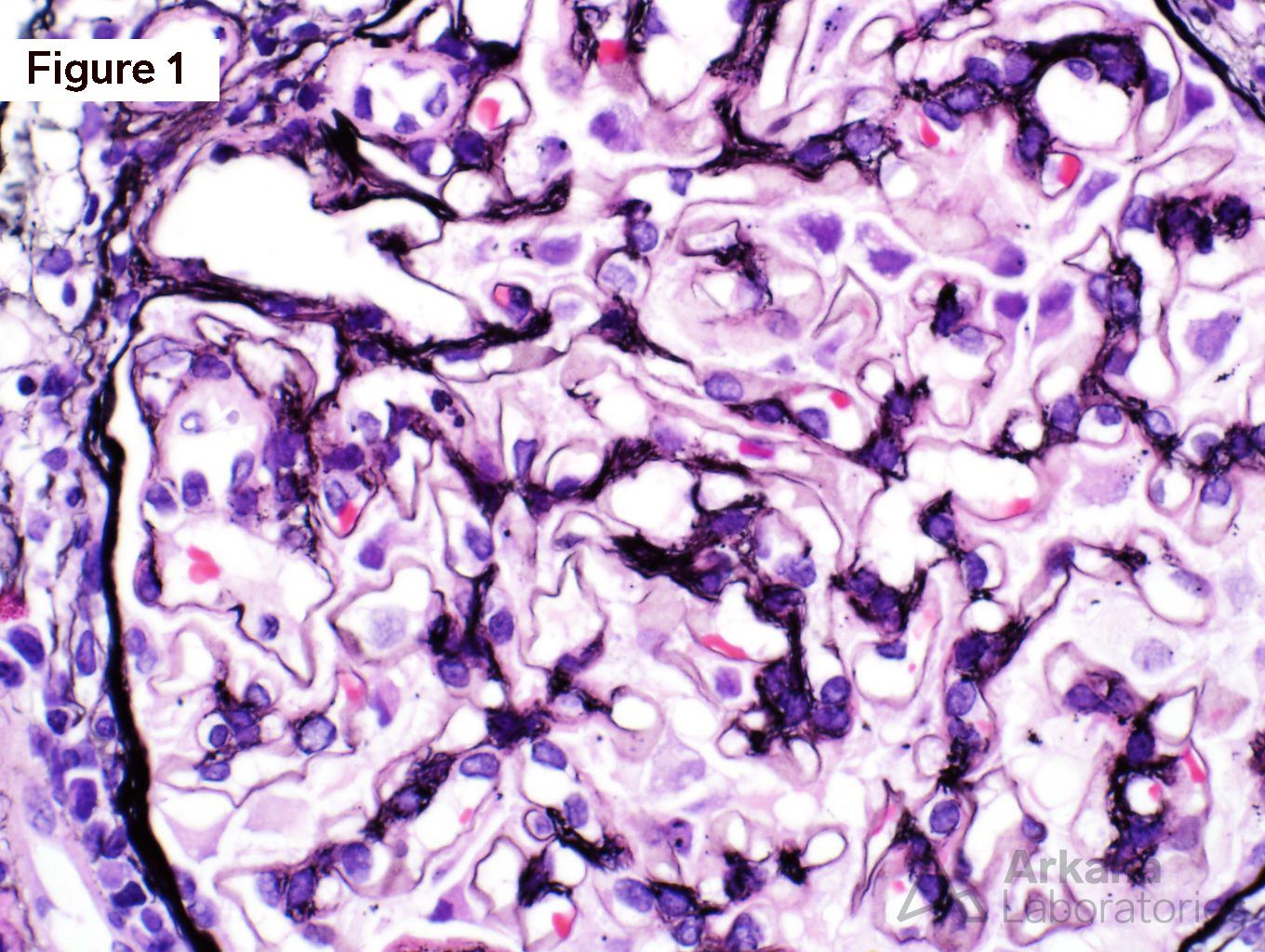
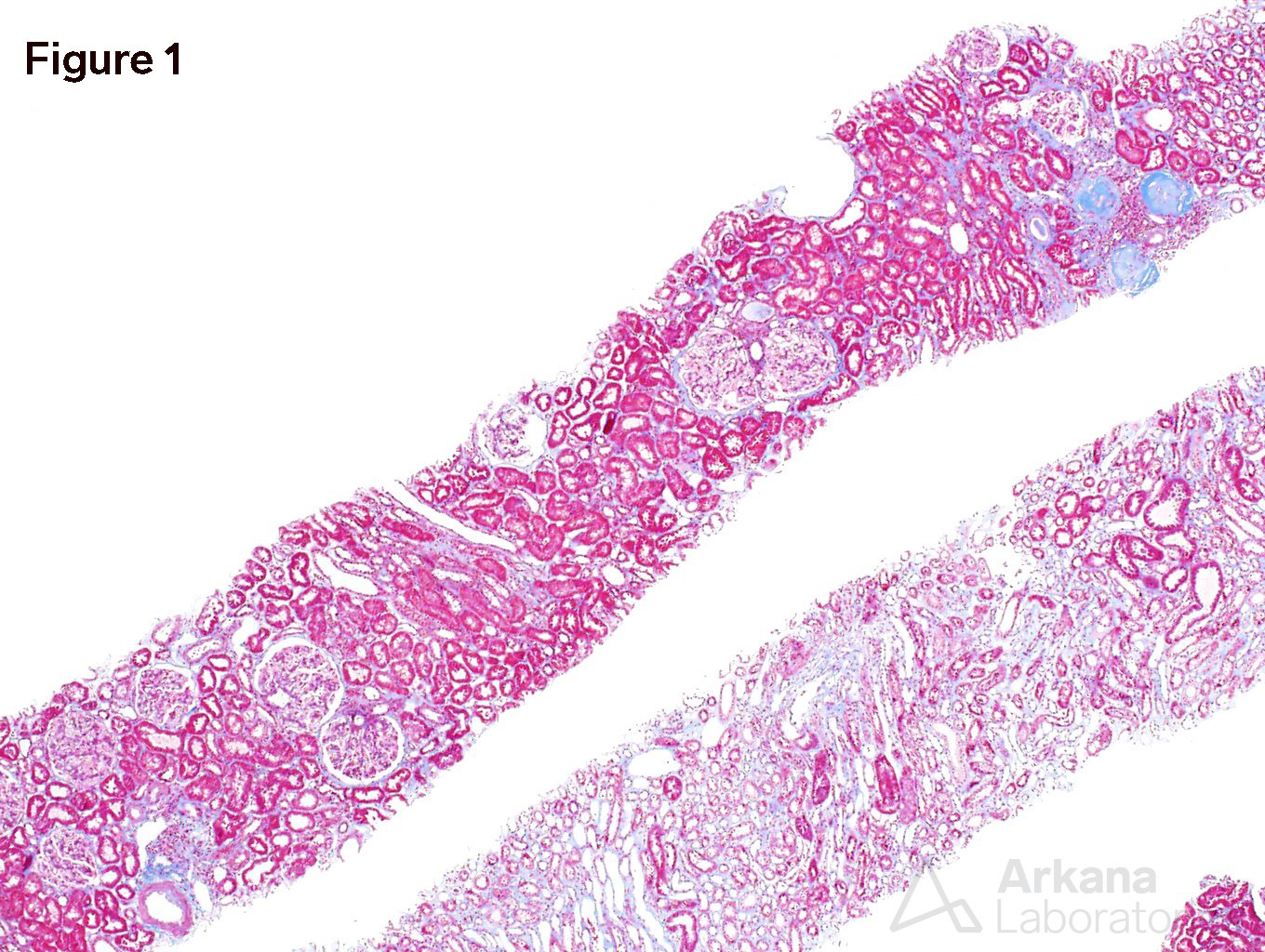
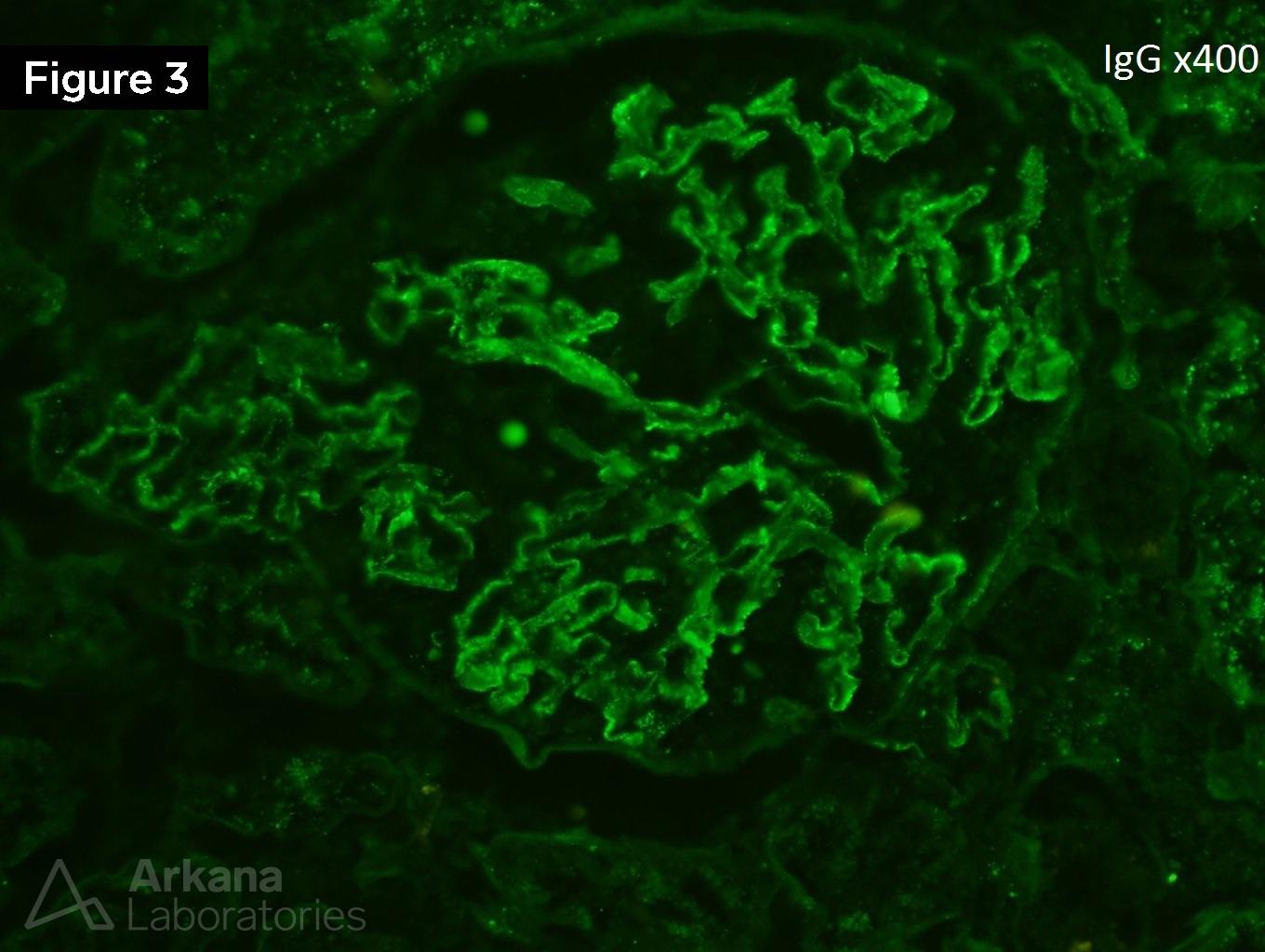
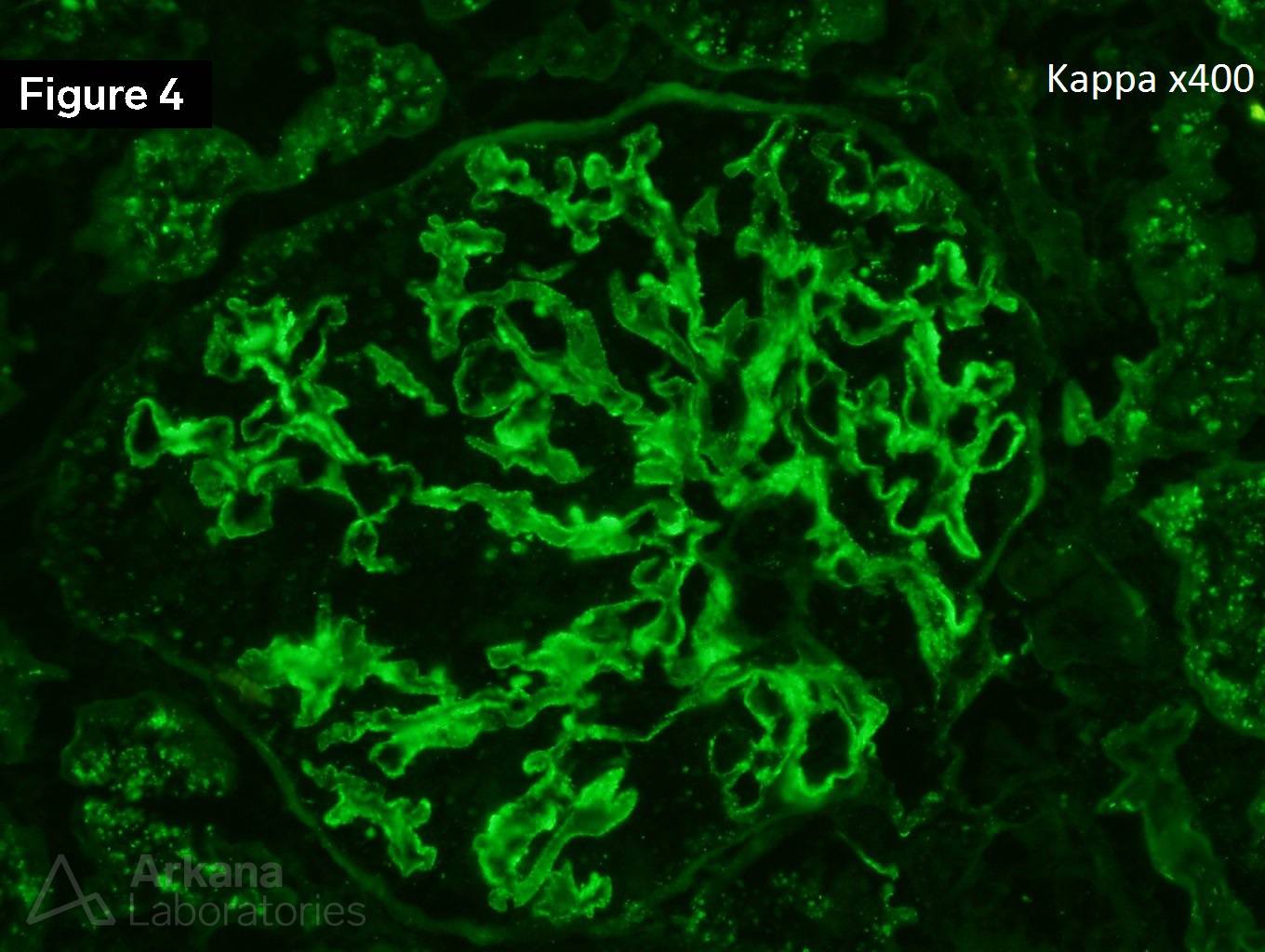
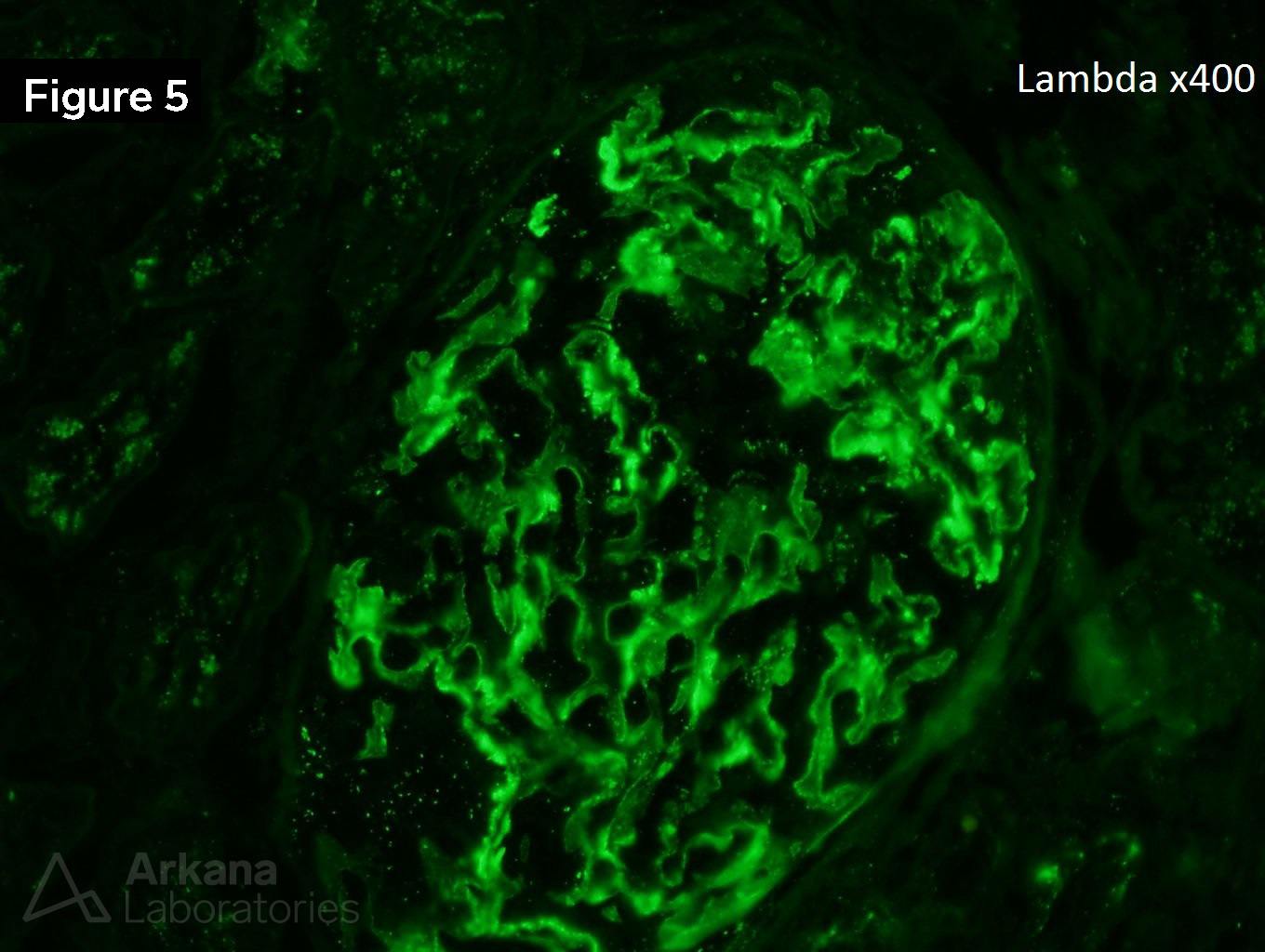
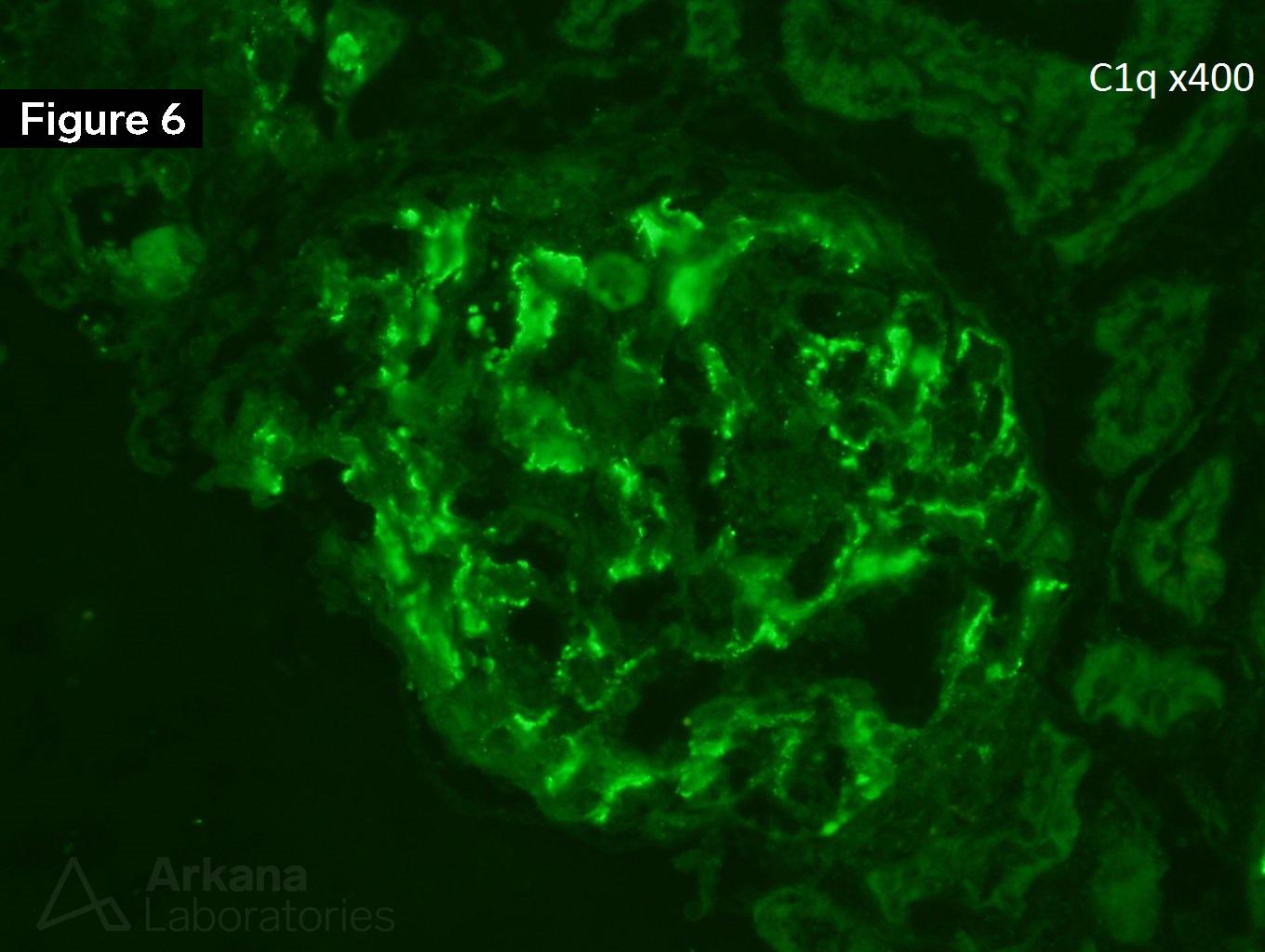
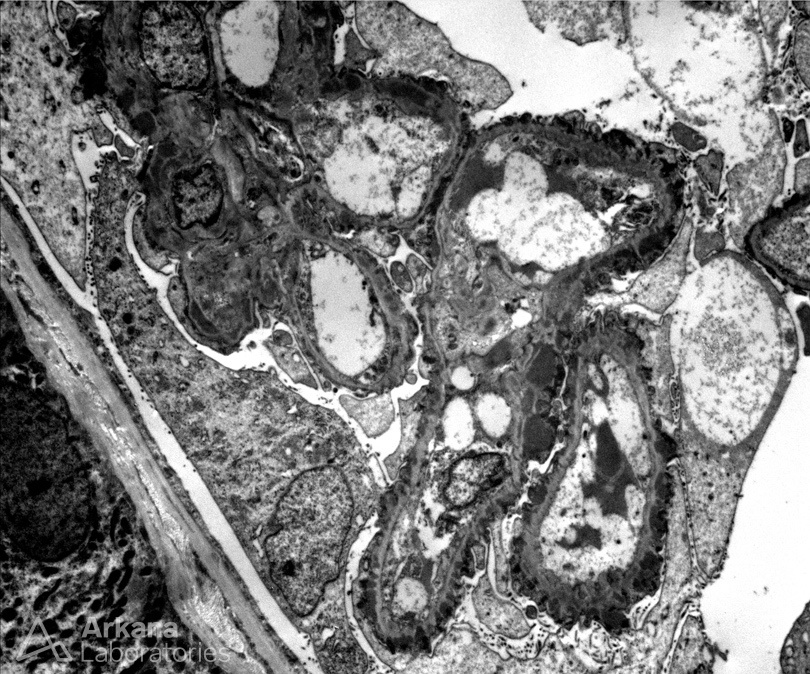
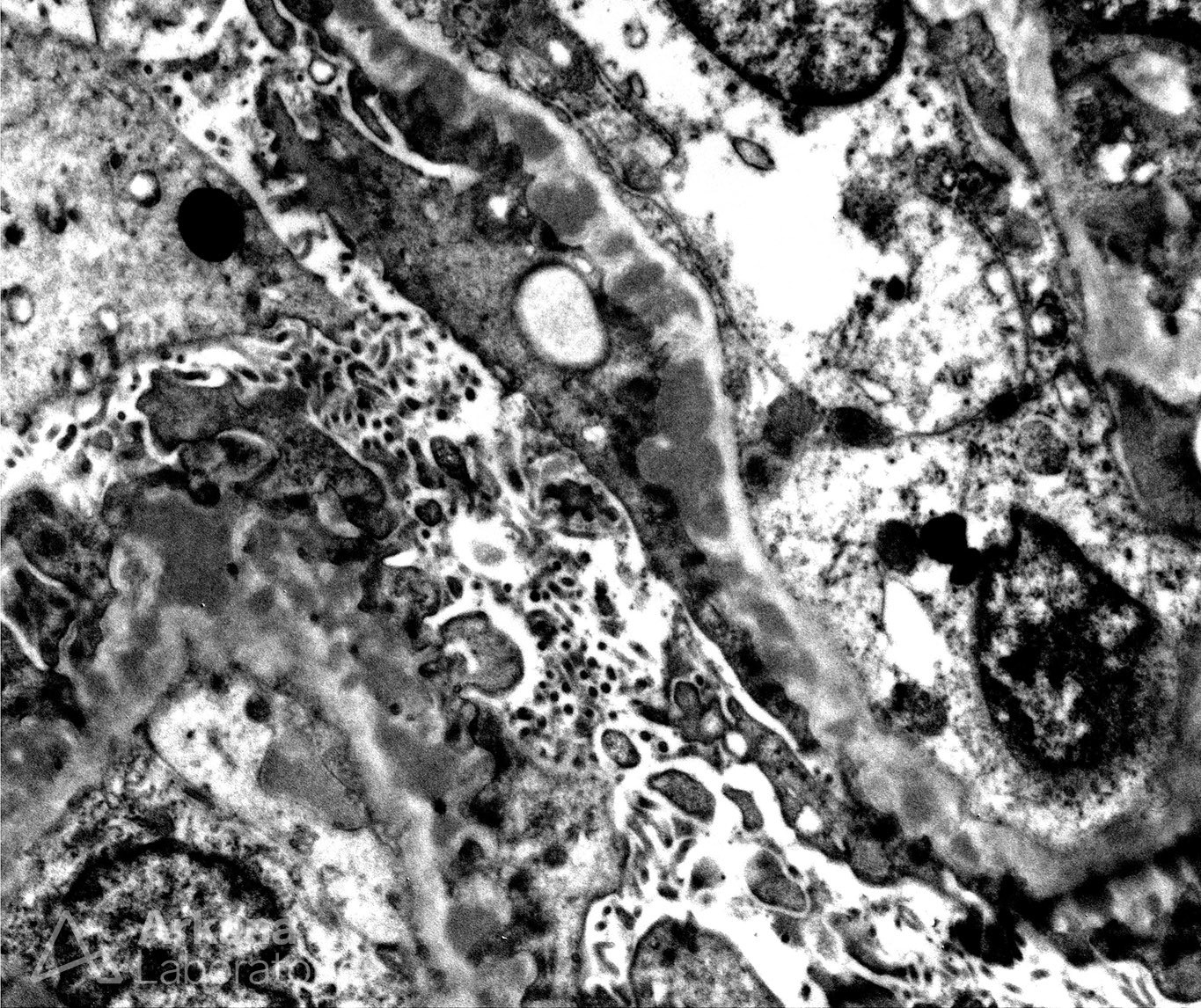
The patient is a 19-year-old female who presents with hematuria, nephrotic range proteinuria, and a creatinine of 1.2 mg/dL. She has a recent diagnosis of systemic lupus erythematosus. Figure 1 shows a normal glomerulus without “spikes” and “holes” of the glomerular basement membranes. Figure 2 shows no significant interstitial fibrosis. Figures 3, 4, 5, & 6 shows IgG, kappa, lambda, and C1q respectively. Image 7 and 8 shows subepithelial deposits.
This is a case of membranous lupus nephritis (ISN/RPS Class V). By definition, no proliferative changes (crescents, fibrinoid necrosis, endocapillary hypercellularity) are seen within the glomeruli in a pure class V membranous lupus nephritis. Although patients with primary membranous nephropathy may have spontaneous remission, those with membranous lupus nephritis do not spontaneously remit. The 2012 ACR Guidelines for Screening, Treatment, and Management of Lupus Nephritis call for MMF as first-line immunosuppression for patients with class V lupus nephritis with nephrotic range proteinuria and/or declining renal function. Rituximab and abatacept have been used off-label for pure class V lesions based on post hoc analyses of studies that included both proliferative and non-proliferative cases of lupus nephritis. A novel calcineurin inhibitor, voclosporin, is currently in phase 3 trials for Class V lupus nephritis. Although direct evidence for the effectiveness of angiotensin inhibition from randomized prospective trials is lacking in patients with membranous lupus nephritis, many clinicians regard angiotensin inhibition as an integral part of routine treatment.
https://www.ncbi.nlm.nih.gov/pubmed/30274623
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.