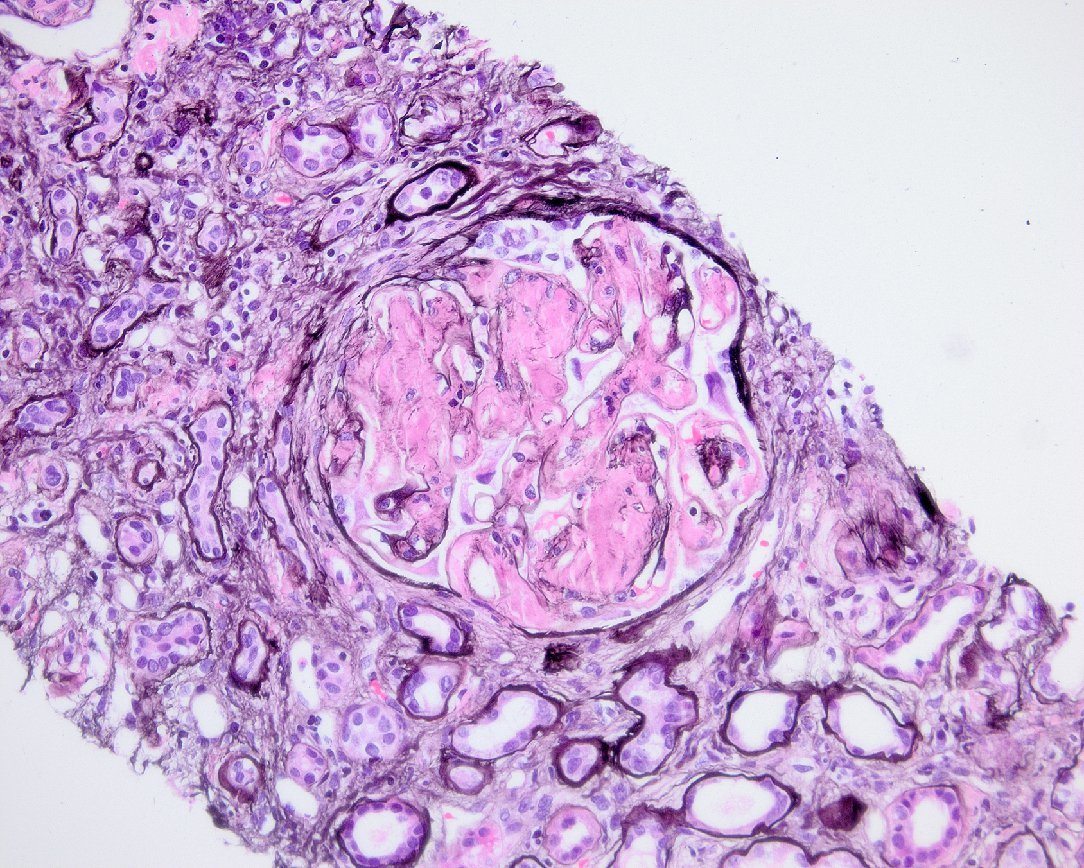
What is your diagnosis in a 35 y/o male with paraplegia and chronic osteomyelitis who presents with nephrotic syndrome? Bonus: What subtype would you suspect based on the clinical history?
The biopsy demonstrates non-argyrophilic material within the mesangium with extension into capillary loops within glomeruli compatible with amyloid deposition. A Congo red stain demonstrated characteristic apple-green birefringence of the material within glomeruli, interstitium, and vascular walls compatible with amyloid. By electron microscopic, the biopsy showed non-branching fibrils averaging 7-10 nm compatible with amyloid. Given the clinical history, the most likely subtype would be AA amyloid as this subtype is usually seen in the setting of chronic inflammatory states and infections (i.e. chronic osteomyelitis). It has also been seen in rheumatoid arthritis, ankylosing spondylitis, inflammatory bowel disease, tuberculosis, familial Mediterranean fever, and in drug users who inject via a subcutaneous route.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.