This 70-year-old patient presented with generalized muscle weakness, weight loss, decreased appetite, mild hypercalcemia, and a 2-month history of progressive right elbow swelling. The patient’s past medical history was significant for gout. Laboratory studies showed elevated ESR (80s-90s). The patient was treated with steroids prior to muscle biopsy and reported significant improvement. Muscle biopsy was performed to evaluate for myopathy.
What is your diagnosis based on Figures #1 through #4?
A. Polymyositis
B. Pyogenic myositis
C. Sarcoidosis
D. B-cell lymphoma
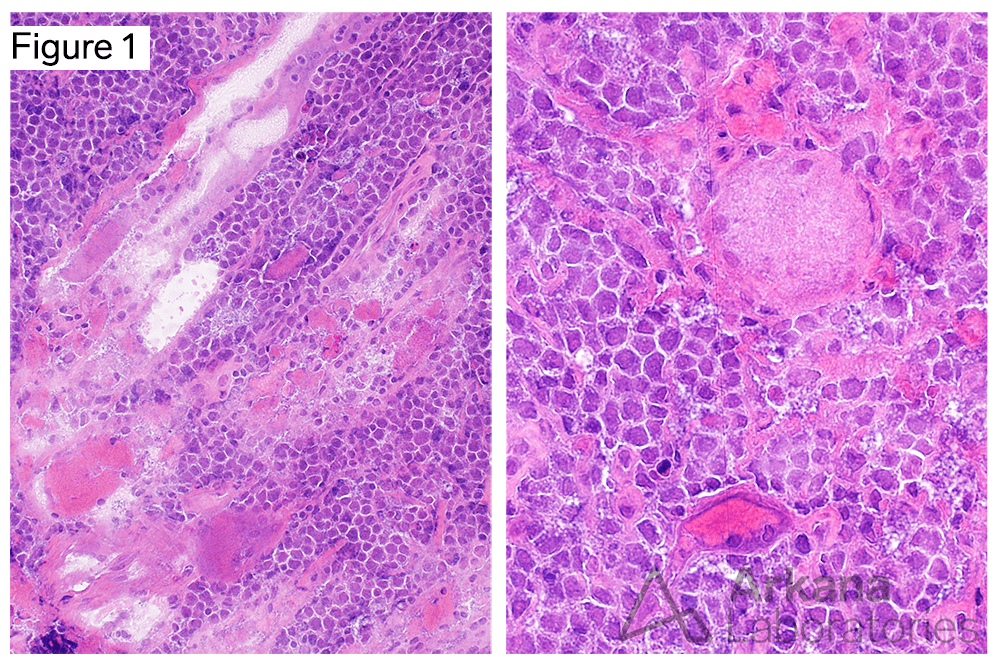
Sections demonstrate the presence of variably atrophic muscle fibers (including basophilic regenerating and necrotic muscle fibers) entrapped within a background cellular infiltrate composed of atypical mononuclear cells with enlarged nuclei and relatively sparse cytoplasm.
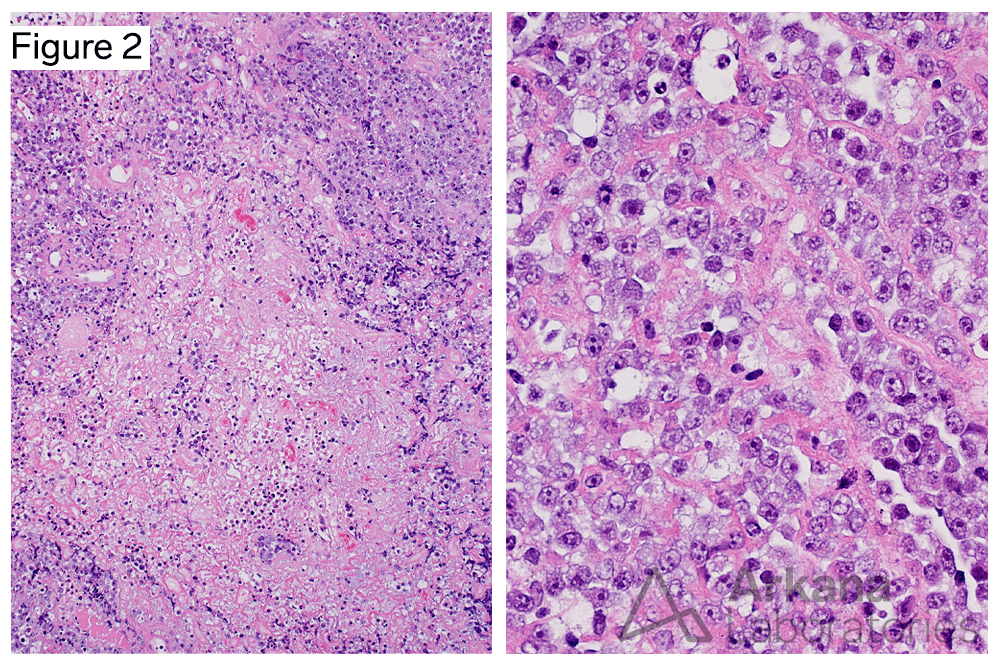
Areas of geographic necrosis are present (left image). The nuclear detail is better demonstrated in formalin-fixed paraffin embedded tissue sections (right image) , and shows that the atypical cells have single to several prominent nucleoli.
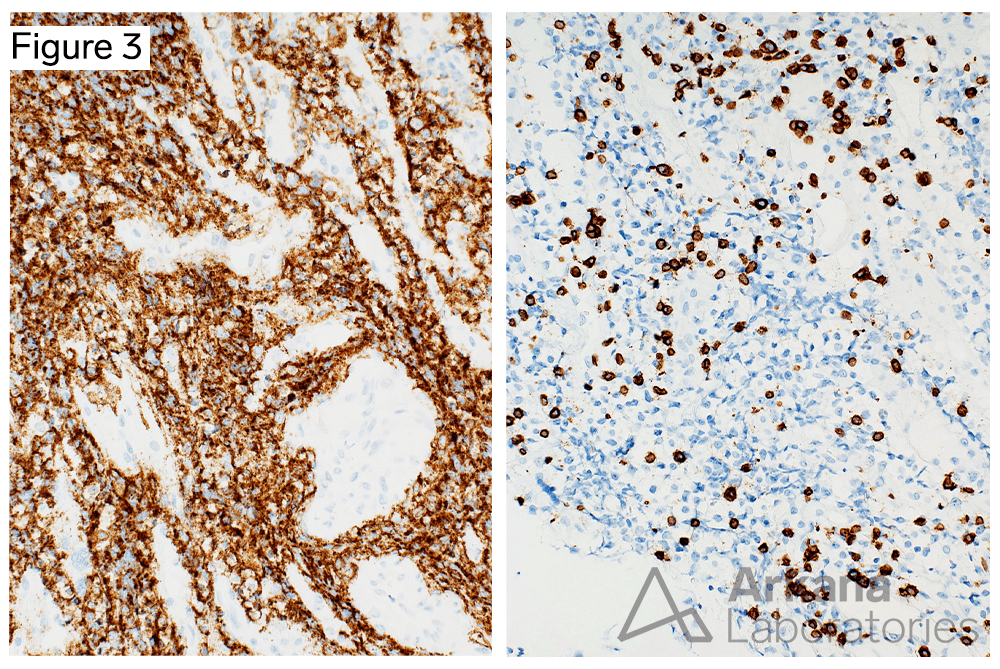
The atypical neoplastic cells show strong diffuse membranous staining for CD20, a marker of B-cell differentiation. Scattered admixed CD3-positive T-cells are present.
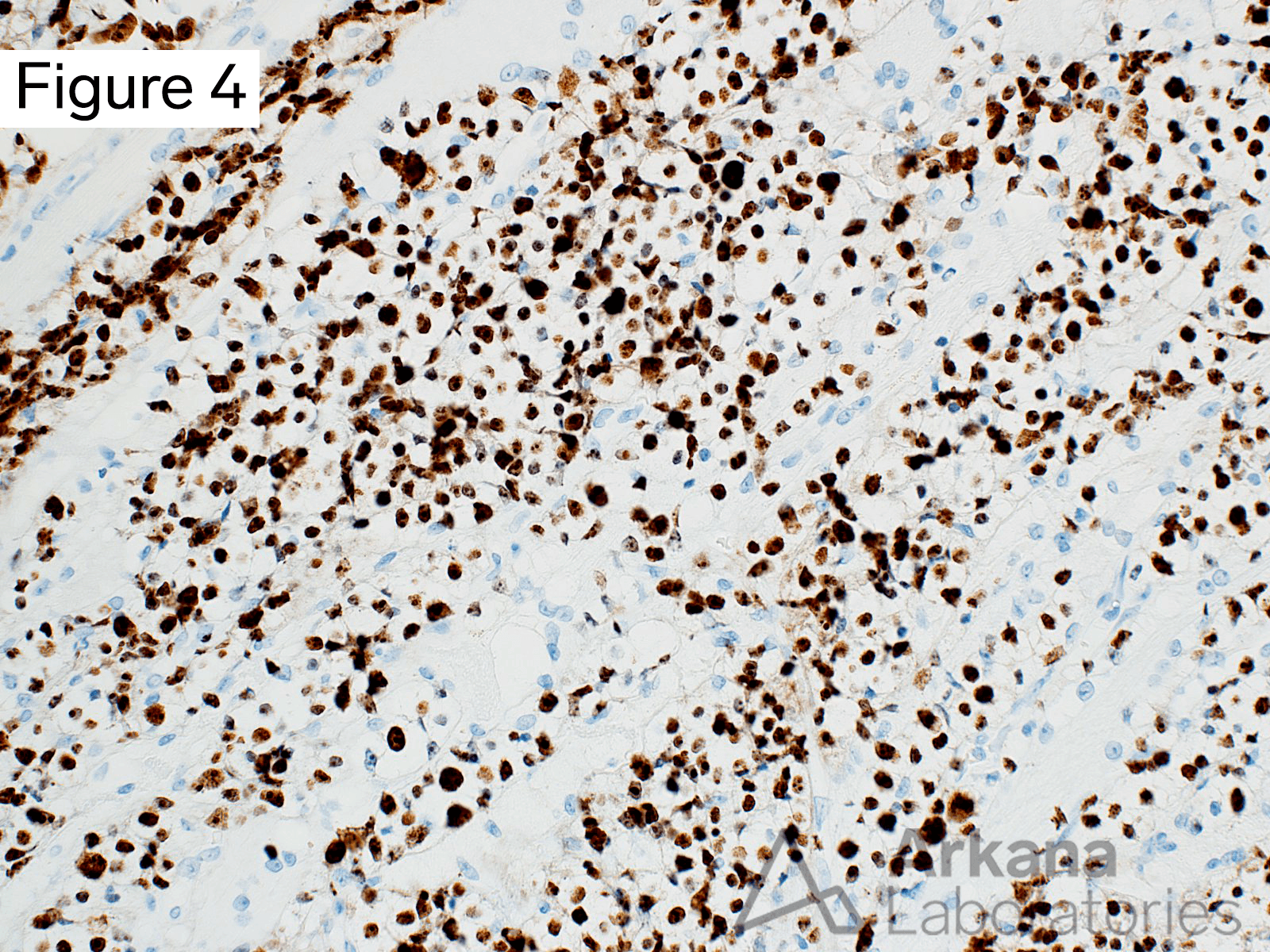
The proliferative fraction, as demonstrated with KI67 (a marker of cell proliferation present in G1, S, G2, and mitotic phases, but absent in G0 resting phase) is very high.
Answer: B-cell lymphoma
The morphologic and immunophenotypic features are consistent with the presence of a “B-cell lymphoma”; specifically Diffuse Large B-cell Lymphoma (DLBCL). Further studies are needed to provide additional prognostic and predictive information, and guide treatment; including immunostains (i.e. Hans algorithm: CD10, BCL6, and MUM1 to determine cell of origin (GCB/germinal center B-cell-like versus ABC/activated B-cell-like subtypes), and Fluorescence In-Situ Hybridiation (FISH) to evaluate for cytogenetic rearrangements involving MYC [IGH-MYC t(8;14)], BCL2 [IGH-BCL2 t(14;18)(q32;q21)], and BCL6 [3q27 gene rearrangement].
More recently DLBCL subtypes are being further investigated using gene expression profiling, next-generation sequencing, and copy number variation type assays.
The lymphoid cells are atypical – rather than mature appearing as would be expected in polymyositis, and are present as a dense infiltrate of B-cells which nearly replaces the skeletal muscle tissue. No neutrophils are seen to suggest that this represents pyogenic/bacterial myositis. Granulomata characteristic of sarcoidosis are not present.
References/Additional Reading
Susanibar-Adaniya S, Barta SK. 2021 Update on Diffuse large B cell lymphoma: A review of current data and potential applications on risk stratification and management. Am J Hematol. 2021 May 1;96(5):617-629. doi: 10.1002/ajh.26151. Epub 2021 Mar 19. PMID: 33661537; PMCID: PMC8172085.
Crombie JL, Armand P. Diffuse Large B-Cell Lymphoma’s New Genomics: The Bridge and the Chasm. J Clin Oncol. 2020 Oct 20;38(30):3565-3574. doi: 10.1200/JCO.20.01501. Epub 2020 Aug 19. PMID: 32813609; PMCID: PMC7571794.
Hans CP, Weisenburger DD, Greiner TC, Gascoyne RD, Delabie J, Ott G, Müller-Hermelink HK, Campo E, Braziel RM, Jaffe ES, Pan Z, Farinha P, Smith LM, Falini B, Banham AH, Rosenwald A, Staudt LM, Connors JM, Armitage JO, Chan WC. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood. 2004 Jan 1;103(1):275-82. doi: 10.1182/blood-2003-05-1545. Epub 2003 Sep 22. PMID: 14504078.
Jeffery GM, Golding PF, Mead GM. Non-Hodgkin’s lymphoma arising in skeletal muscle. Ann Oncol. 1991 Jul;2(7):501-4. doi: 10.1093/oxfordjournals.annonc.a058002. PMID: 1911457.
Binici DNR, Karaman A, Timur O, Tasar PNT, Sanibas AV. Primary skeletal muscle lymphoma: A case report. Mol Clin Oncol. 2018 Jan;8(1):80-82. doi: 10.3892/mco.2017.1483. Epub 2017 Nov 3. PMID: 29387400; PMCID: PMC5768100.
Spetsieris N, Giannakopoulou N, Variami E, Zervakis K, Rougala N, Garefalakis G, Skarlatou V, Viniou NA, Diamantopoulos P. Isolated skeletal muscle recurrence of an originally nodal diffuse large B cell lymphoma: A case report and review of the literature. Medicine (Baltimore). 2018 Jan;97(3):e9608. doi: 10.1097/MD.0000000000009608. PMID: 29504987; PMCID: PMC5779756.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.