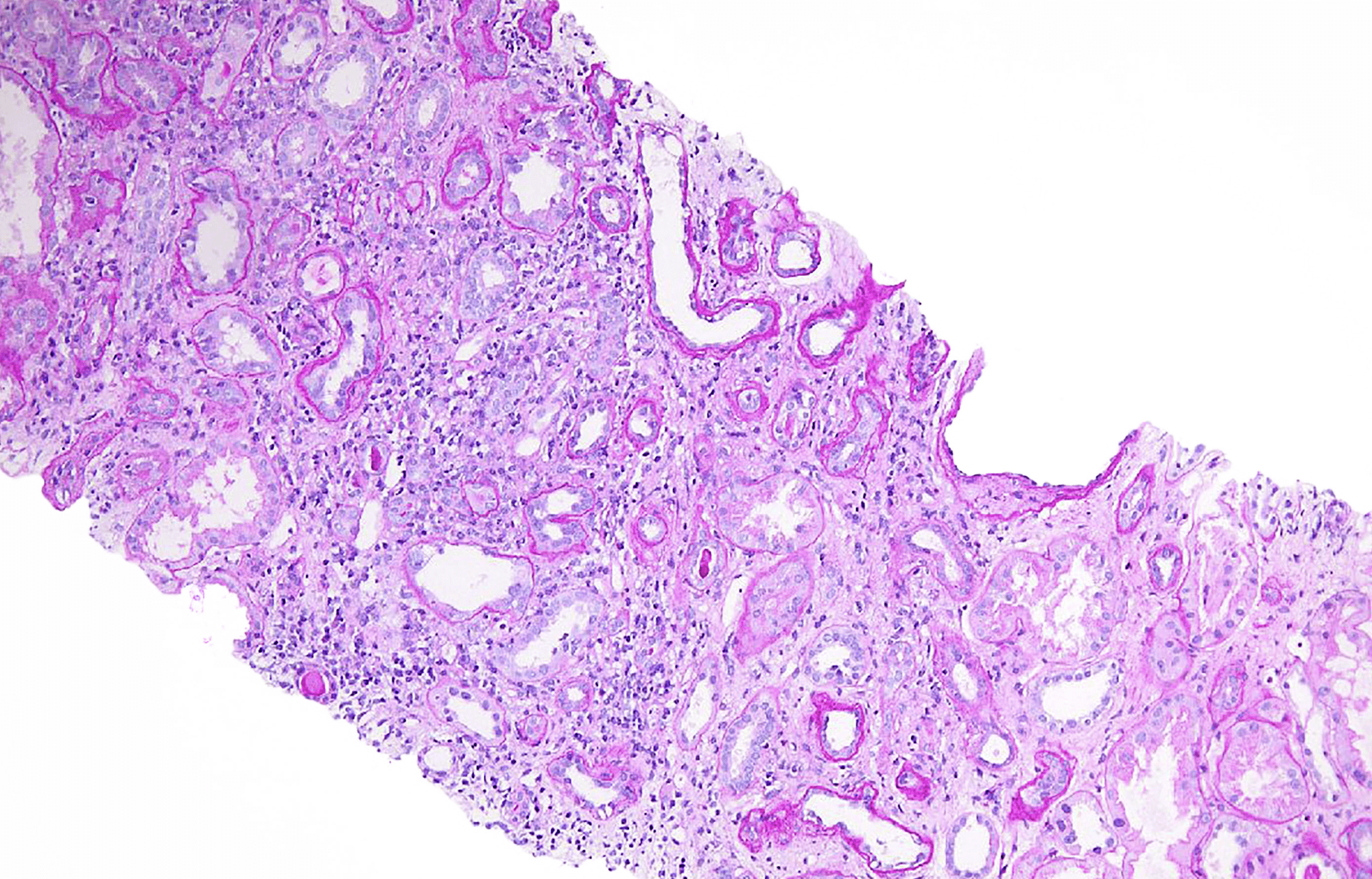
In Episode 6 of Banff and Beyond, our patient is a 55 y/o male status post deceased donor renal transplant approximately 2 years ago who now presents with increased creatinine. As we can see from the biopsy, there is predominately lymphoplasmacytic interstitial inflammation as well as areas of tubular atrophy. Additionally, intact tubules show significant tubular injury characterized by epithelial simplification and reactive nuclear changes as well as areas demonstrating epithelial sloughing and apoptotic debris. There were also intact tubules demonstrating mild lymphocytic tubulitis; thus, at first glance, this constellation of findings is concerning for T cell-mediated rejection. However, as we continue to look at intact tubules we can see that some of the tubular nuclei demonstrate a somewhat “glassy” cleared-out appearance compatible with viral cytopathic effect. Sure enough, upon examination of our SV40 stain, we can see that these nuclei are positive and upon discussion with the nephrologist, he was known to have a positive BK viral titer. Thus, the biopsy demonstrates polyomavirus nephropathy, PVN class II given positive staining in 1-10% of tubular nuclei along with moderate tubular atrophy and interstitial fibrosis.
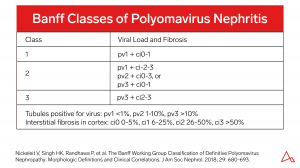
For further information on polyomavirus nephropathy, please see the PVN classification scheme below as well as an associated reference. Reference: Nickeleit V, Singh HK, Randhawa P, et al. The Banff Working Group Classification of Definitive Polyomavirus Nephropathy: Morphologic Definitions and Clinical Correlations. J Am Soc Nephrol. 2018; 29: 680-693.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.