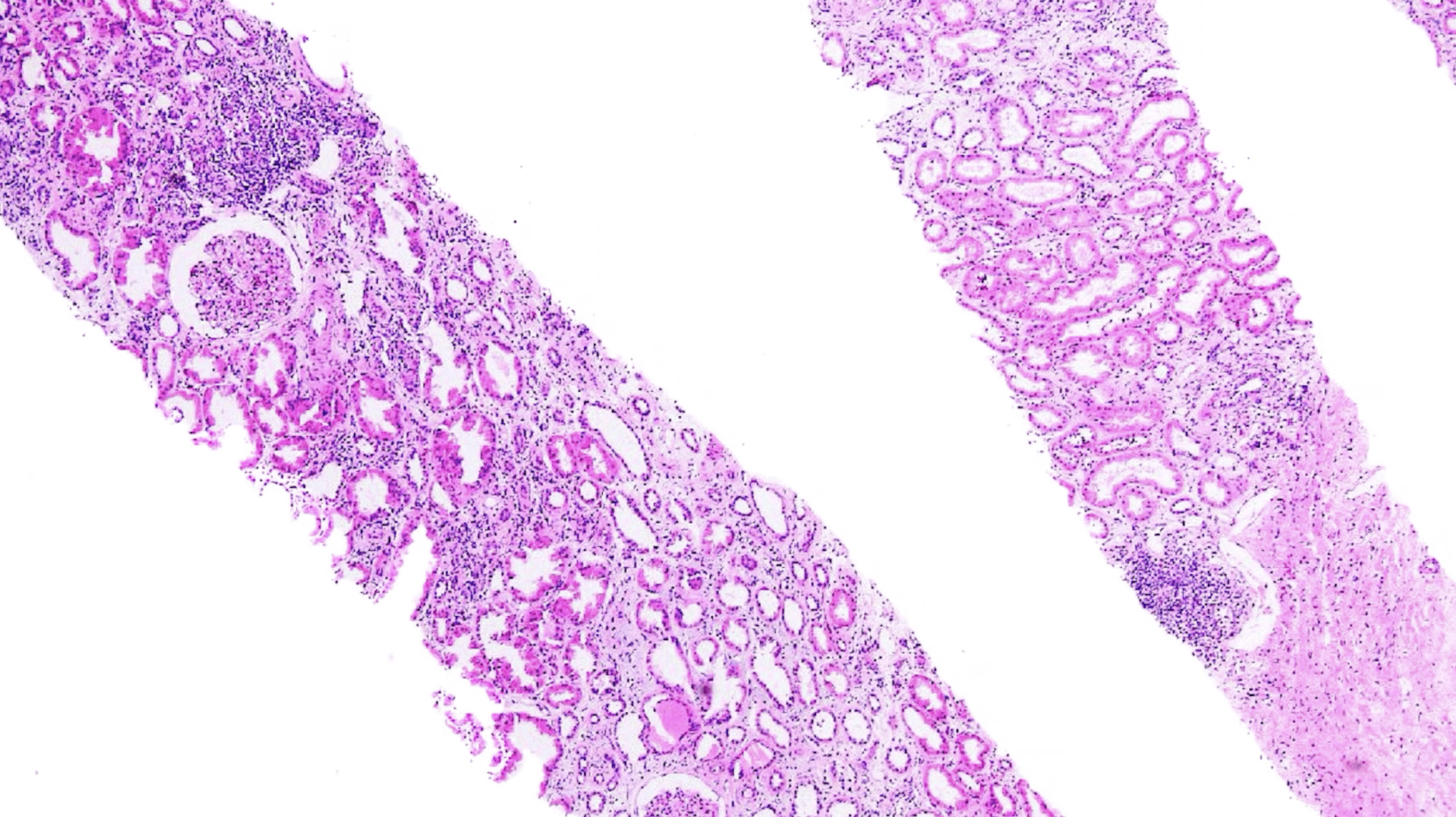
Welcome back to the third installment of our transplant series, Banff and Beyond. In this episode, Dr. Murphy continues the discussion on transplant rejection. The patient today is a 72 y/o male status post deceased donor renal transplant ~1.5 yrs. ago. He presents with AKI and reports spitting his immunosuppressive medications and intermittent use. The biopsy demonstrates histologic features of acute T-cell mediated rejection, Banff grade IA, as it shows predominately lymphocytic interstitial inflammation with approximately 30-40% of the unscarred cortex (Banff score: I2) along with moderate lymphocytic tubulitis within multiple non-atrophic tubules (Banff score: T2). As discussed in prior episodes, tubulitis is ideally graded in tubules cut in cross-section; however, if a longitudinally cut tubule is used, it is scored as the number of mononuclear cells per ten tubular epithelial cells. It is important to remember that severely atrophic tubules, including those with endocrine type atrophy, a diameter of less than 25% of the unaffected tubules, or those with pronounced basement membrane wrinkling or thickening, should not be utilized for the evaluation of possible tubulitis.
For reference categories of interstitial inflammation and tubulitis scores as follows:
I0 (<10%), I1 (10-25%), I2 (26-50%), I3 (>50%)
T1 (1-4 cells), T2 (5-10 cells), and T3 (>10 cells).
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.