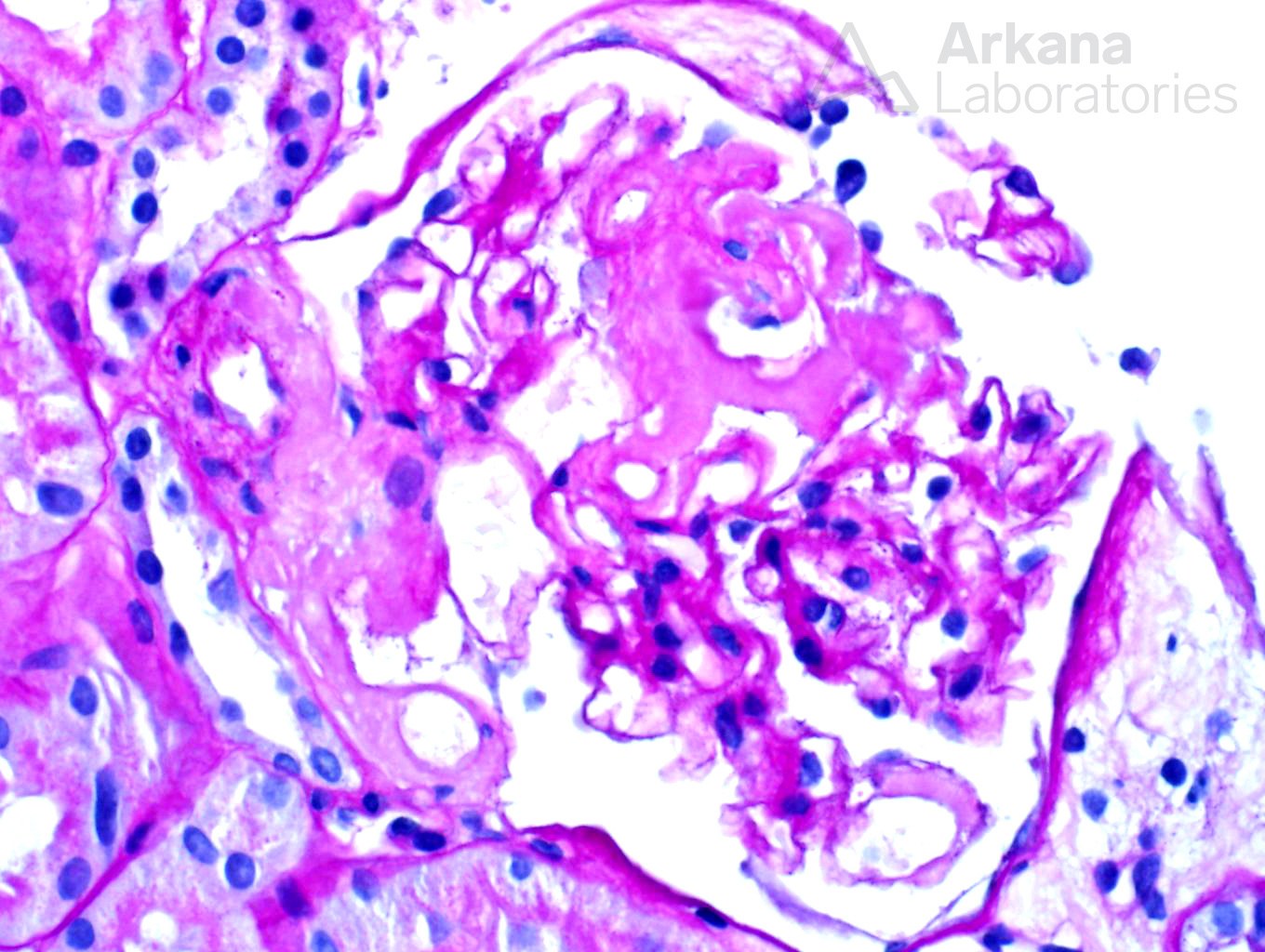
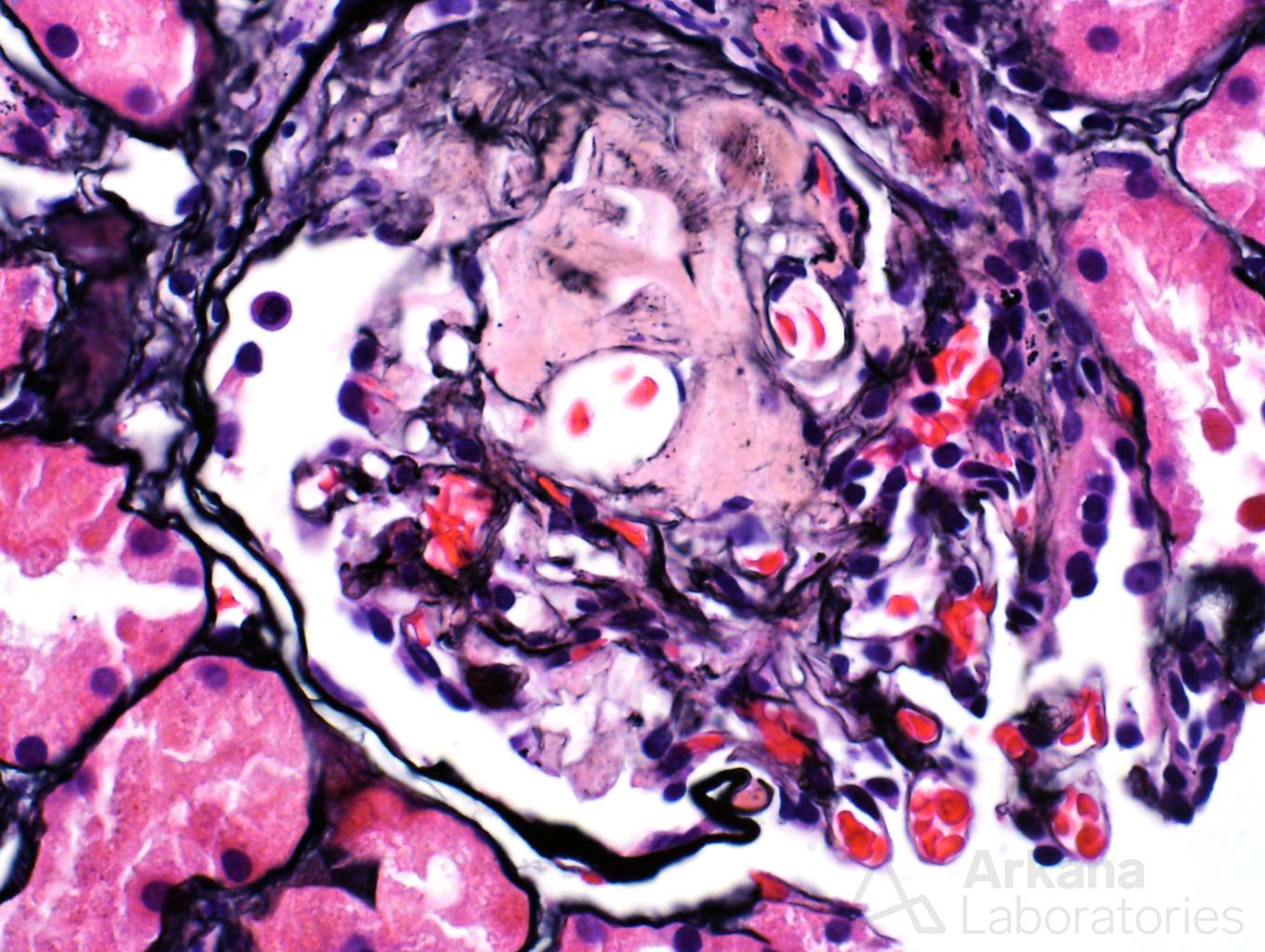
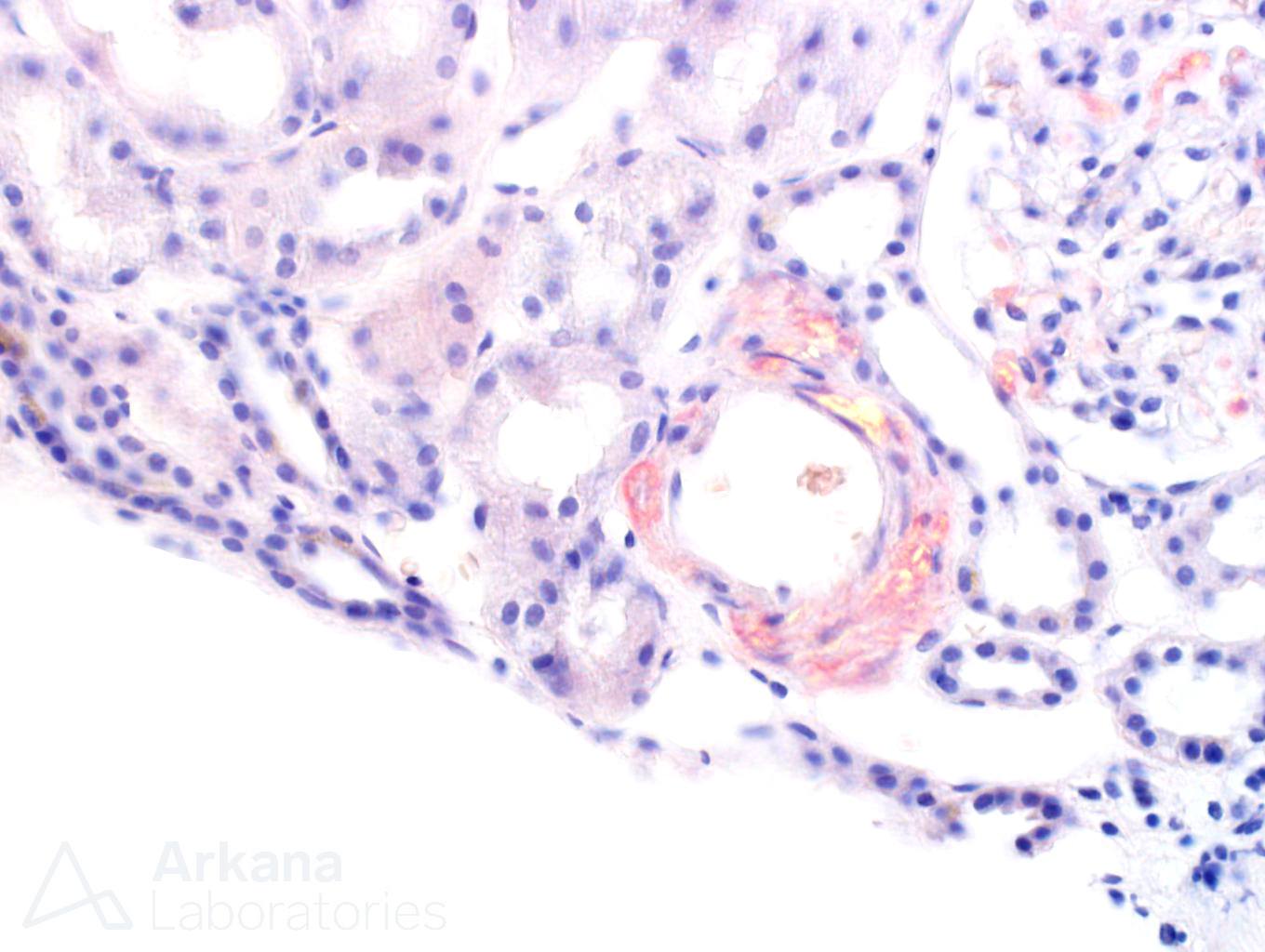
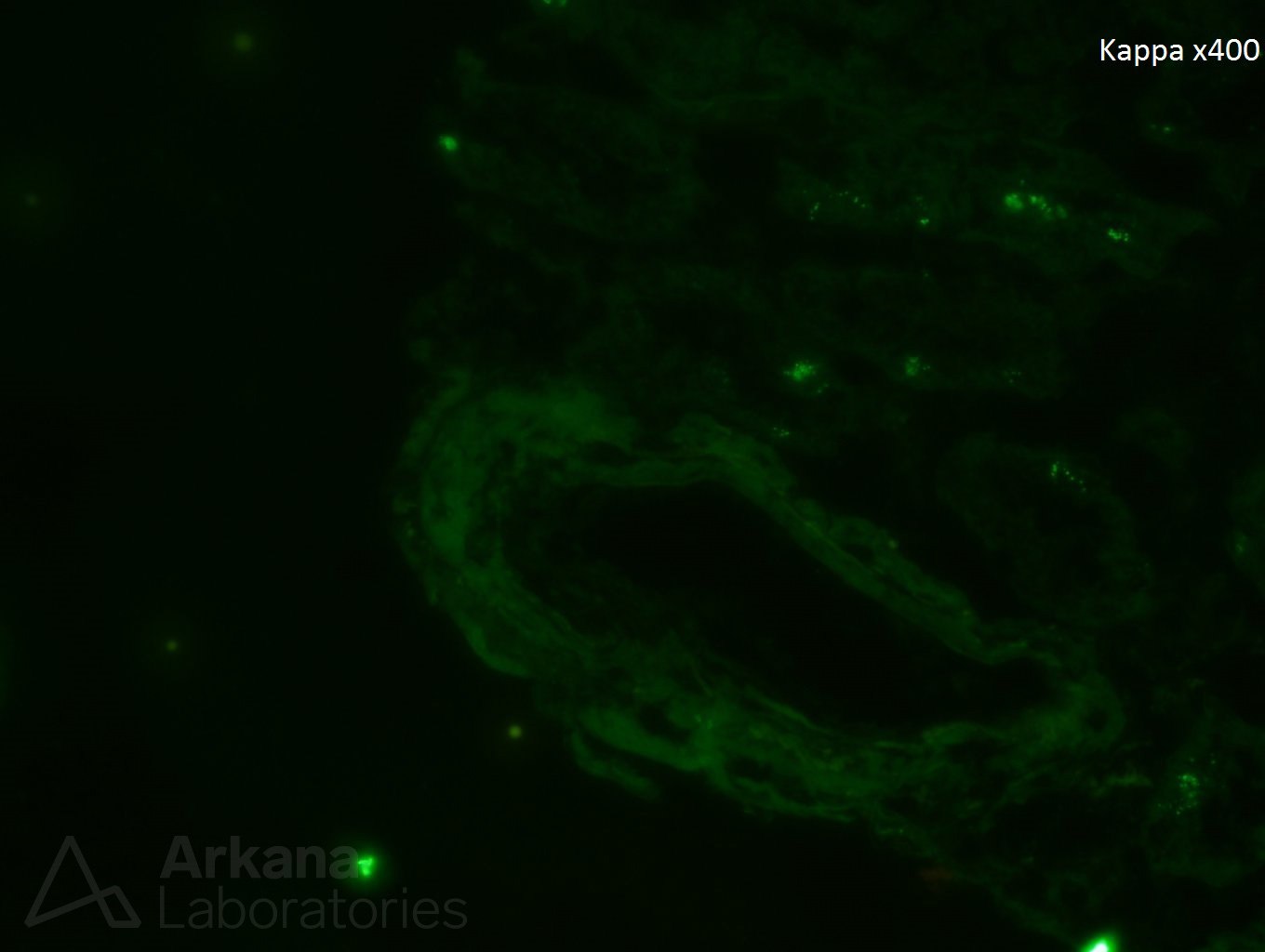
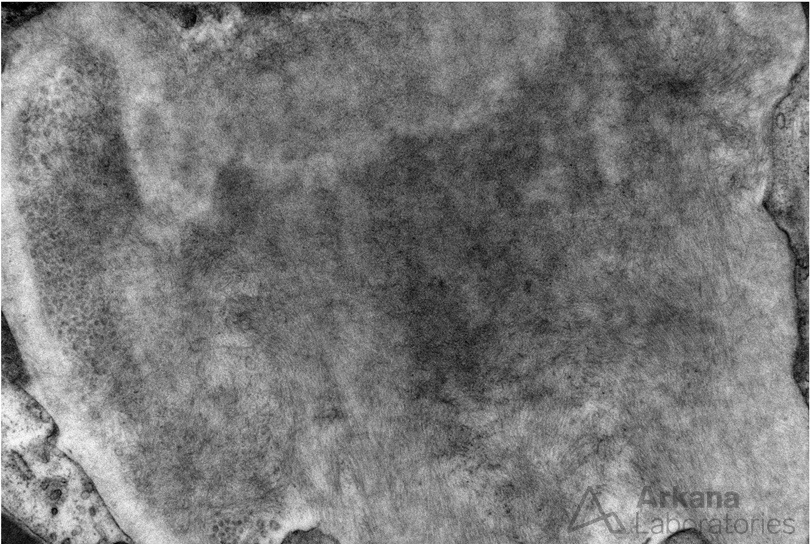
A 70 year-old female presents with nephrotic range proteinuria and a creatinine of 1.2. She was in her normal level of health until about 6 months ago when she noticed foamy urine and swelling in her ankles. She has lost 30 lbs unintentionally during the last few months. Her cardiologist said that her proteinuria does not appear to be related to the heart. A kidney biopsy is performed. The glomerulus in figure 1 is distorted and has a “washed-out” or pale appearance on PAS stain. A silver stain shows material which is non-argyrophilic (figure 2). A Congo red stain shows apple-green birefringence within this material (figure 3). Immunofluorescence stain shows negative staining for kappa (figure 4) and bright staining with lambda (figure 5) within a vessel wall. Electron microscopy confirms the presence of non-branching fibrils within this material (figure 6).
Amyloidosis is a known cause of proteinuria. The immunofluorescence staining confirms the presence of a restricted, pathologic light chain from an underlying plasma cell dyscrasia. AL-type amyloidosis results from extracellular tissue deposition of misfolded immunoglobulin light chain fragments. AL-type amyloidosis is the most common cause of amyloidosis in the western hemisphere and a monoclonal protein is detectable in urine and/or serum in >95% of affected patients by immunofixation or measurements of serum free light chains. This type of amyloidosis usually affects multiple organ systems and treatment is typically directed at eradication of the underlying plasma cell dyscrasia.

Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.