Clinical presentation
The patient is a 45-year-old male with a history of IV drug use, hepatitis C, and multiple skin abscesses who presents with proteinuria and renal failure.
Kidney biopsy findings
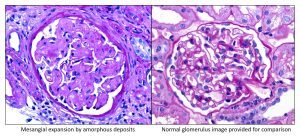
The main finding on kidney biopsy is shown in Figure 1 (PAS stain). The patient’s biopsy is on the left. On the right is a normal glomerulus for comparison. In the patients’ biopsy, an amorphous material expands the mesangium, giving the glomerulus a vaguely nodular appearance. Note that the deposits show weak PAS staining.
Differential for mesangium expansion by deposits
Mesangial expansion by deposits raises several possibilities listed below. The staining pattern of the deposits on PAS and Silver stains can help in differentiating the etiology.
- Diabetes mellitus – strong PAS staining, silver positive.
- Light/heavy chain – strong PAS staining, silver negative.
- Amyloid – weak PAS staining, silver negative.
- Fibrillary – strong PAS staining, silver negative.
Additional clues
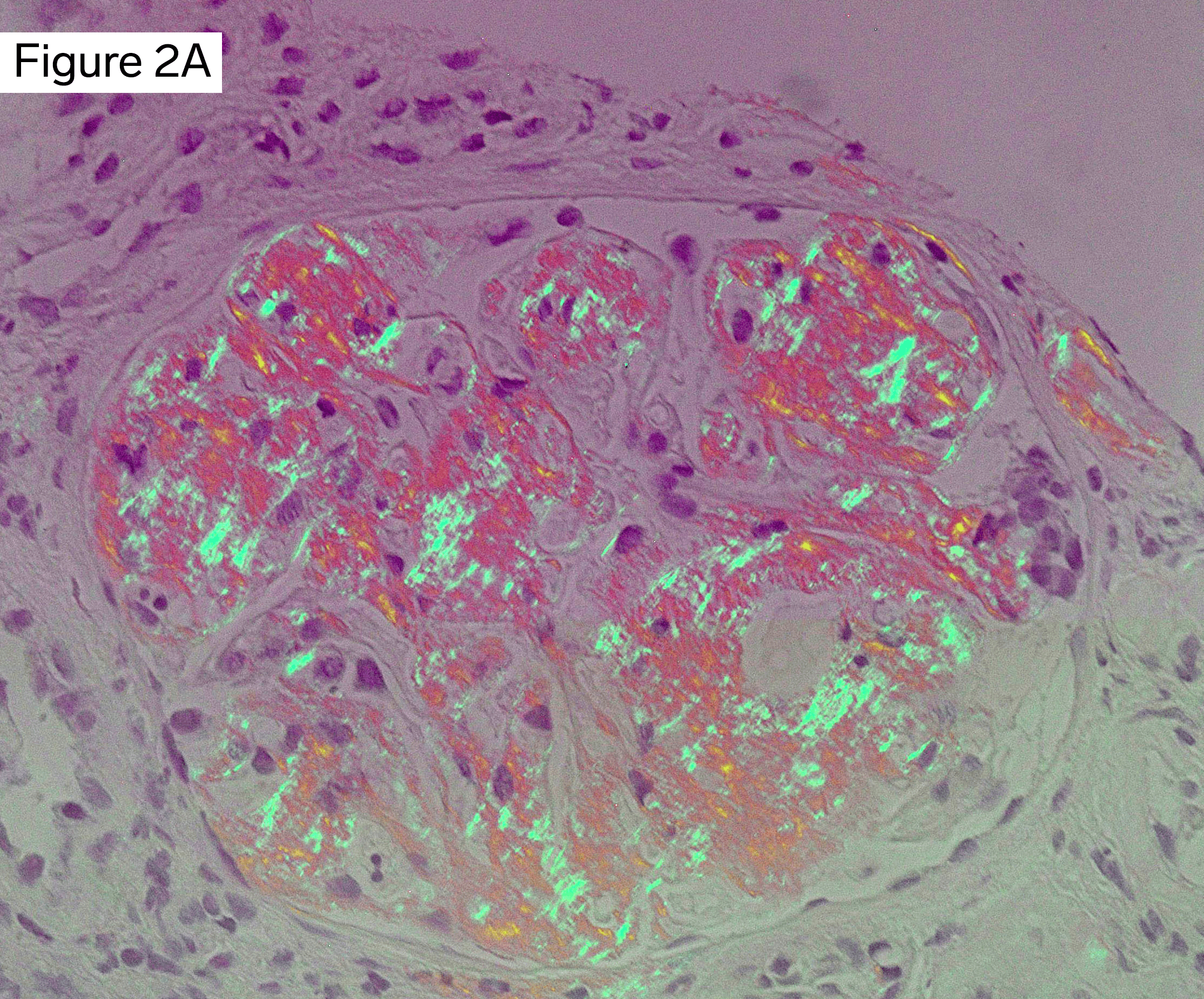
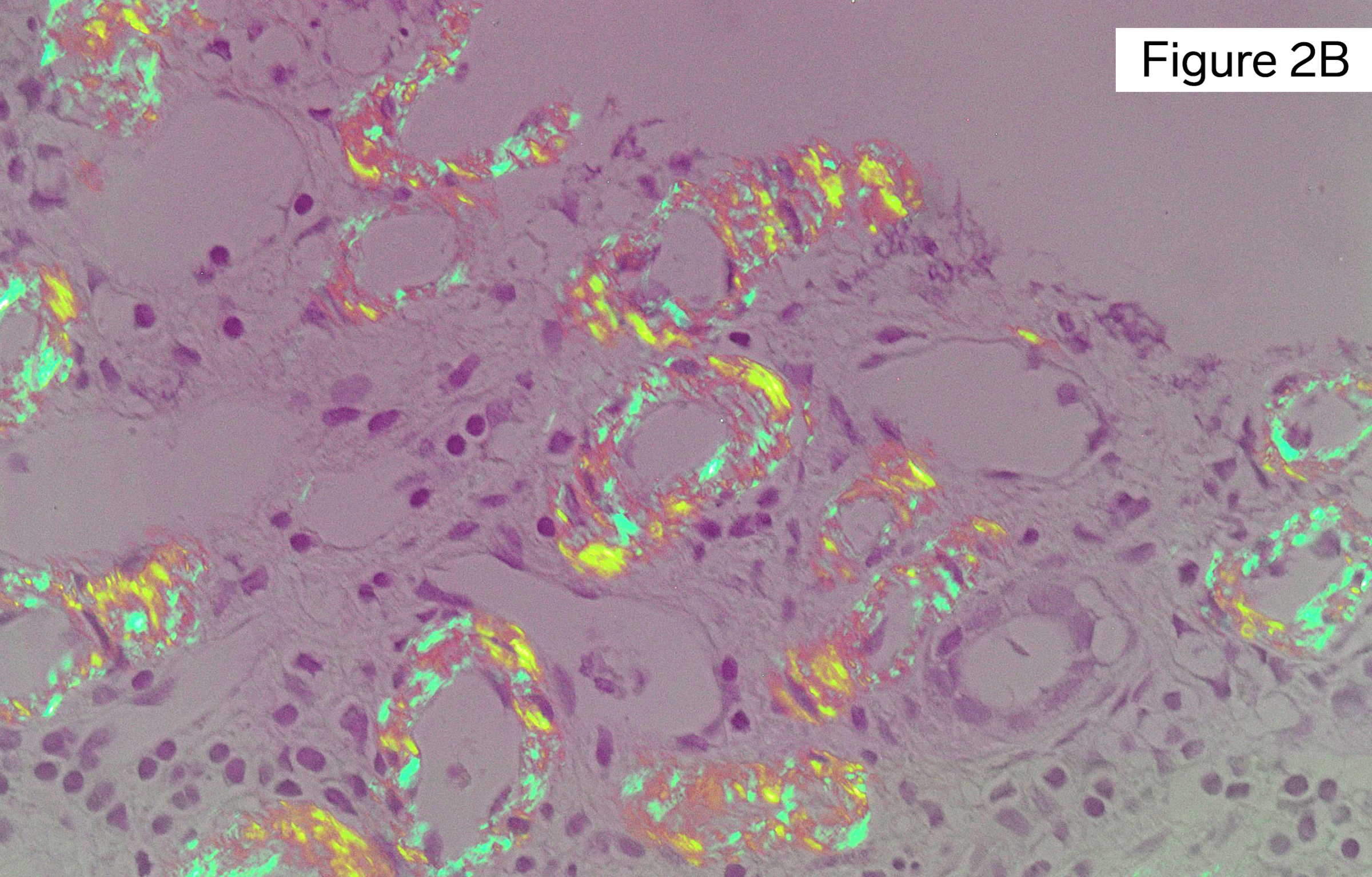
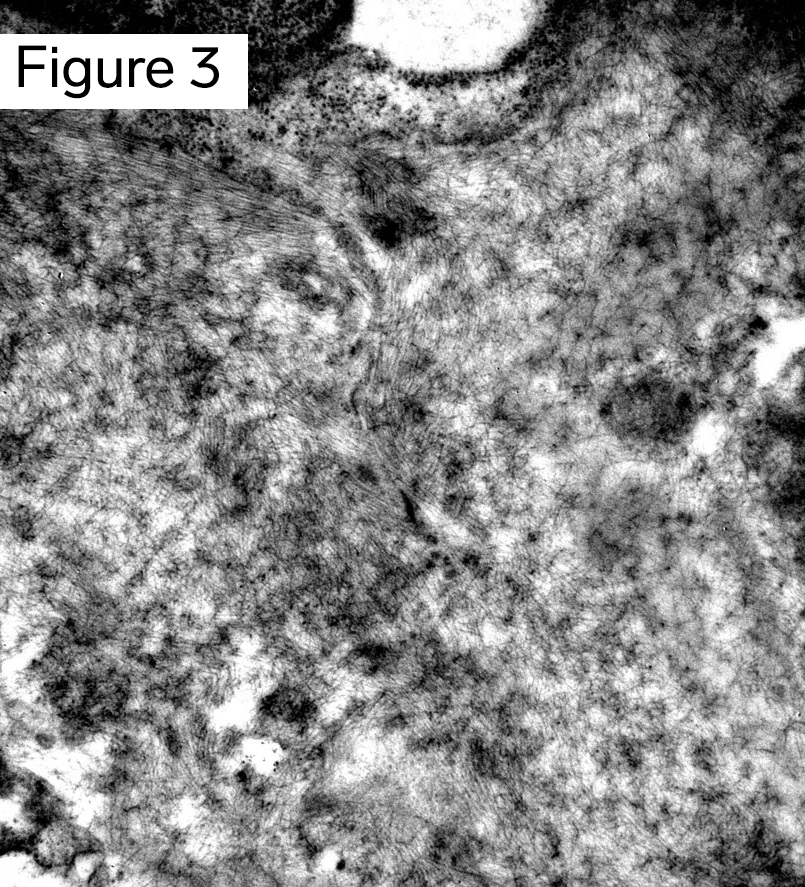
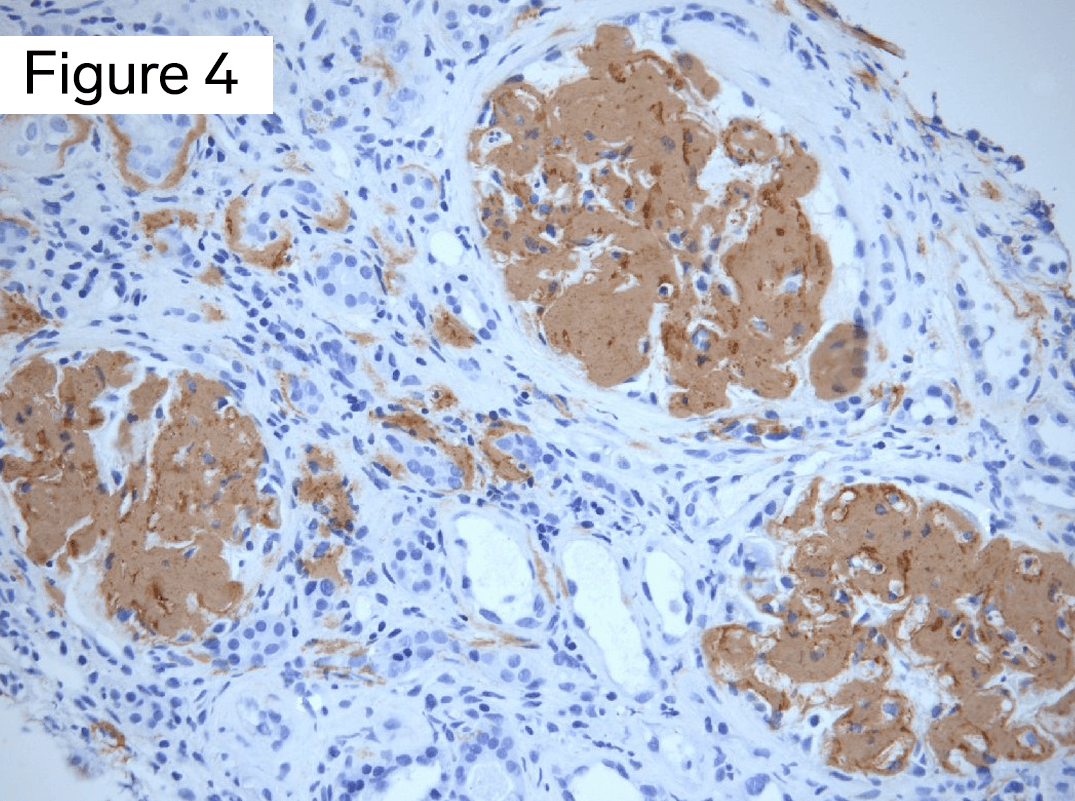
The deposits stain positive on Congo red with apple-green birefringence upon polarization, Figure 2A. There is also tubulointerstitial and vascular involvement, Figure 2B. On electron microscopy, nonbranching fibrils 10 nm in diameter are identified, Figure 3. The deposits stain positive on immunohistochemical stain for serum amyloid A protein, Figure 4.
What is the diagnosis?
In summary, the kidney biopsy of a patient with a history of IV drug use and chronic infections shows weak PAS staining of mesangial amyloid. Testing for serum amyloid A protein by immunohistochemistry is positive. Taken together, the diagnosis is Amyloidosis, AA type. Amyloidosis is caused by deposition of abnormal misfolded proteins with beta-pleated sheet configuration. Examination by Congo red stain with polarized light is the gold standard technique to detect amyloid. A positive test for amyloid shows apple-green birefringence. On electron microscopy, randomly arranged fibrils 7-12 nm in diameter are seen.
As many as 30 different amyloid proteins have been described. The most common type is AL amyloid, from immunoglobulin light chains. Other types include amyloid formed from serum amyloid A protein (AA), transthyretin (ATTR), and leukocyte chemotactic factor 2 (LECT2). Testing for amyloid protein type is done by immunofluorescence, immunohistochemistry or mass spectrometry. AA amyloidosis, due to the deposition of serum amyloid A protein, usually takes many years to develop. Serum amyloid A protein is an acute phase reactant associated with chronic infection. This fits with the patient’s history of drug use and hepatitis C. The patient’s multiple skin abscesses is likely from “skin popping”, where drugs are deposited under the skin.
References
Colvin, Robert, B. and Anthony Chang. Diagnostic Pathology: Kidney Diseases. Available from: Elsevier eBooks+, (3rd Edition). Elsevier – OHCE, 2019.
Jennette JC, Olson JL, Silva FG, D’Agati V, Heptinstall RH *1920 *, eds. Heptinstall’s Pathology of the Kidney: Includes Interactive EBook with Complete Content. Seventh edition. Wolters Kluwer; 2015.
Larsen CP, Walker PD, Weiss DT, Solomon A. Prevalence and morphology of leukocyte chemotactic factor 2-associated amyloid in renal biopsies. Kidney International. 2010;77(9):816-819.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.