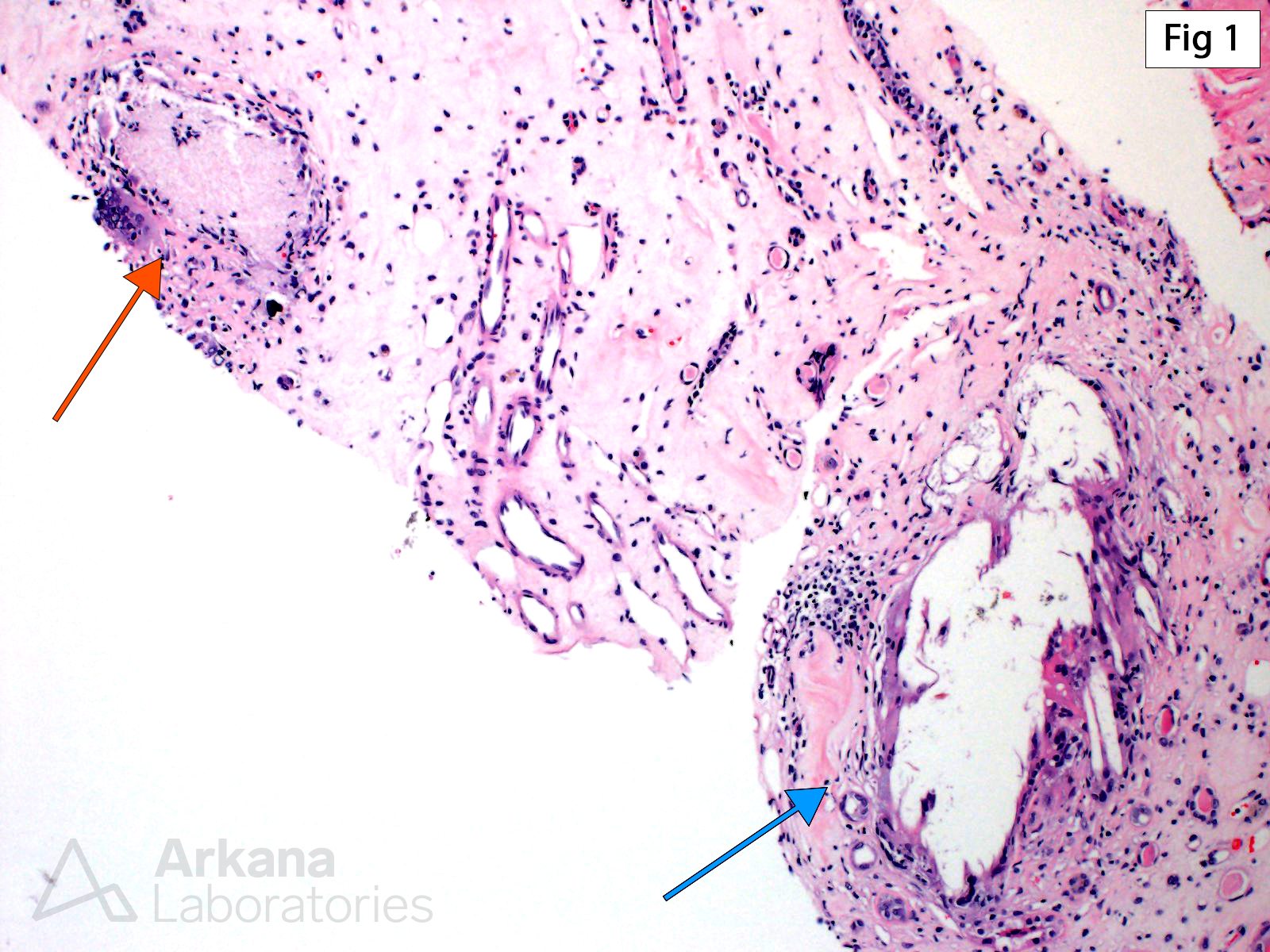
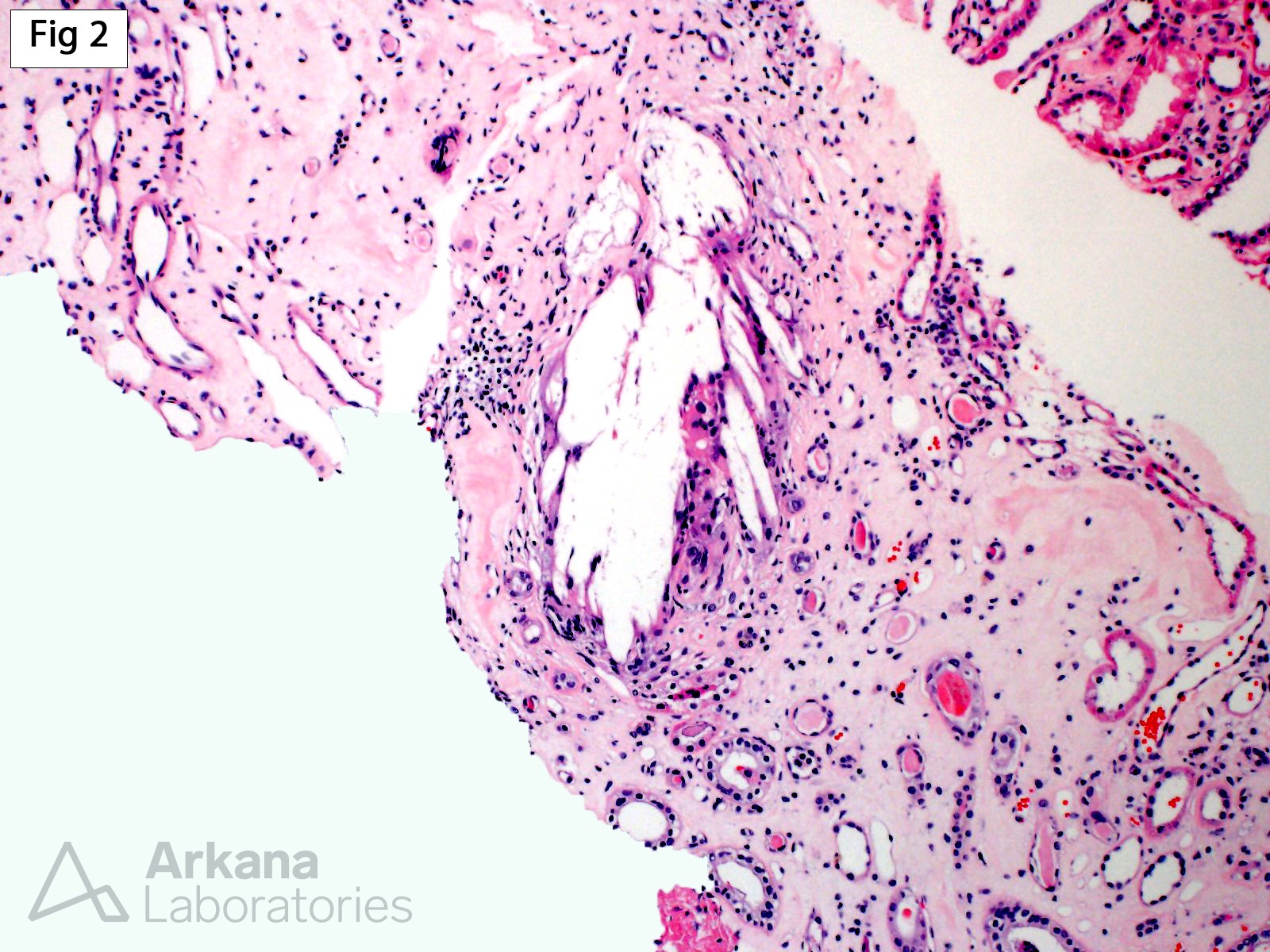
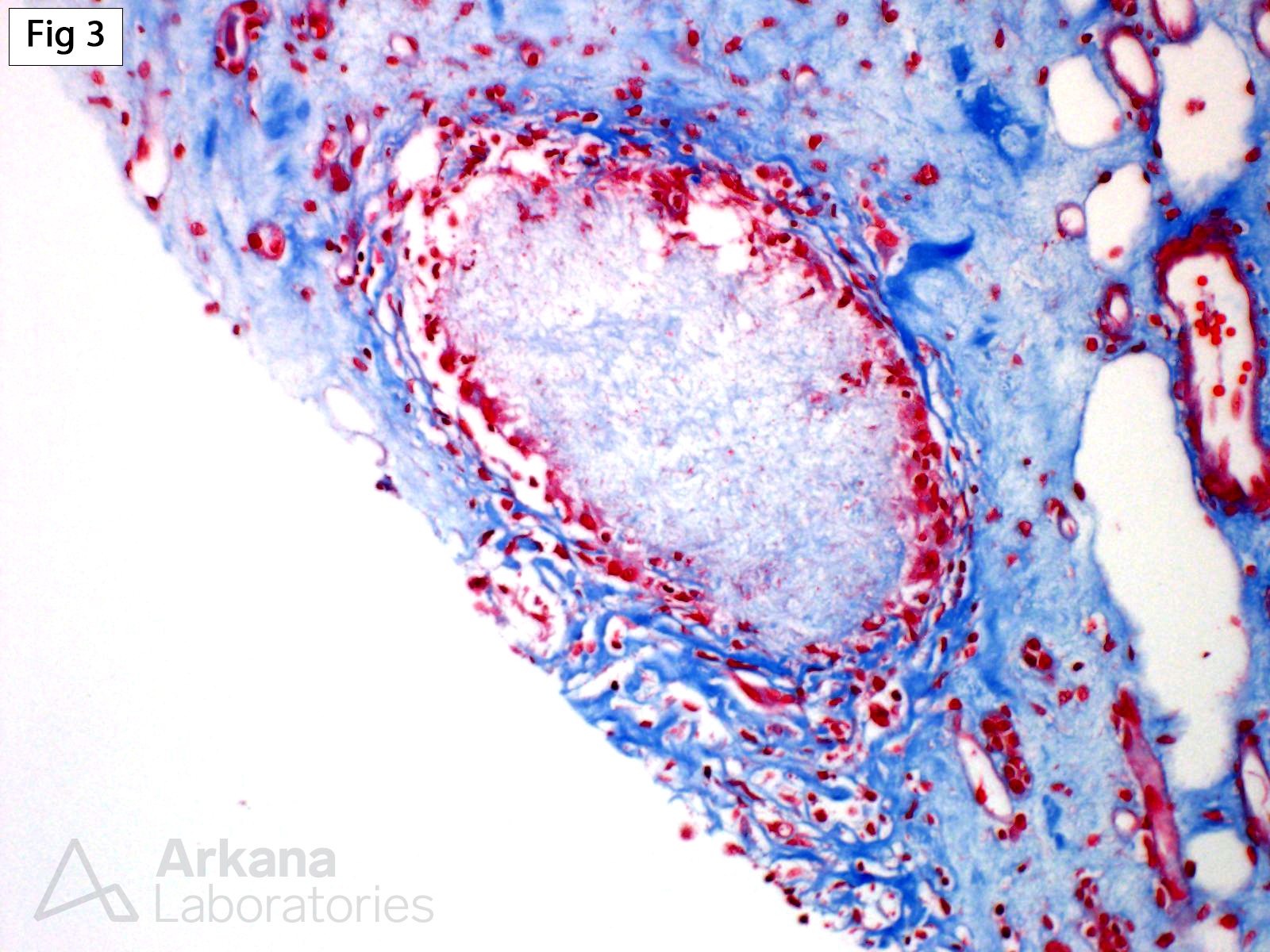
Chronic uric acid nephropathy results from deposition within the renal parenchyma of monosodium urate monohydrate. While the disease may occur in the setting of increased uric acid production, it is overwhelmingly more common in the setting of decreased uric acid excretion. Histologically, chronic uric acid nephropathy is characterized by the presence of tubulointerstitial microtophi within the renal medulla, associated with interstitial fibrosis and inflammation. Microtophi are deposits of monosodium urate crystals surrounded by giant cells, epithelioid histiocytes, and lymphocytes, which may have a radial needle-like cleft (Fig 1 – blue arrow; Fig 2) or amorphous morphology (Fig 1 – orange arrow; Fig 3 [trichrome]). While the crystals are dissolved during formalin fixation, their birefringence is readily seen on frozen or alcohol-fixed tissue. In addition to the tubulointerstitial changes, the glomeruli may show mesangial sclerosis, thickening of the glomerular basement membranes, and segmental subendothelial widening by electron microscopy.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.