Focal crescentic IgA nephropathy
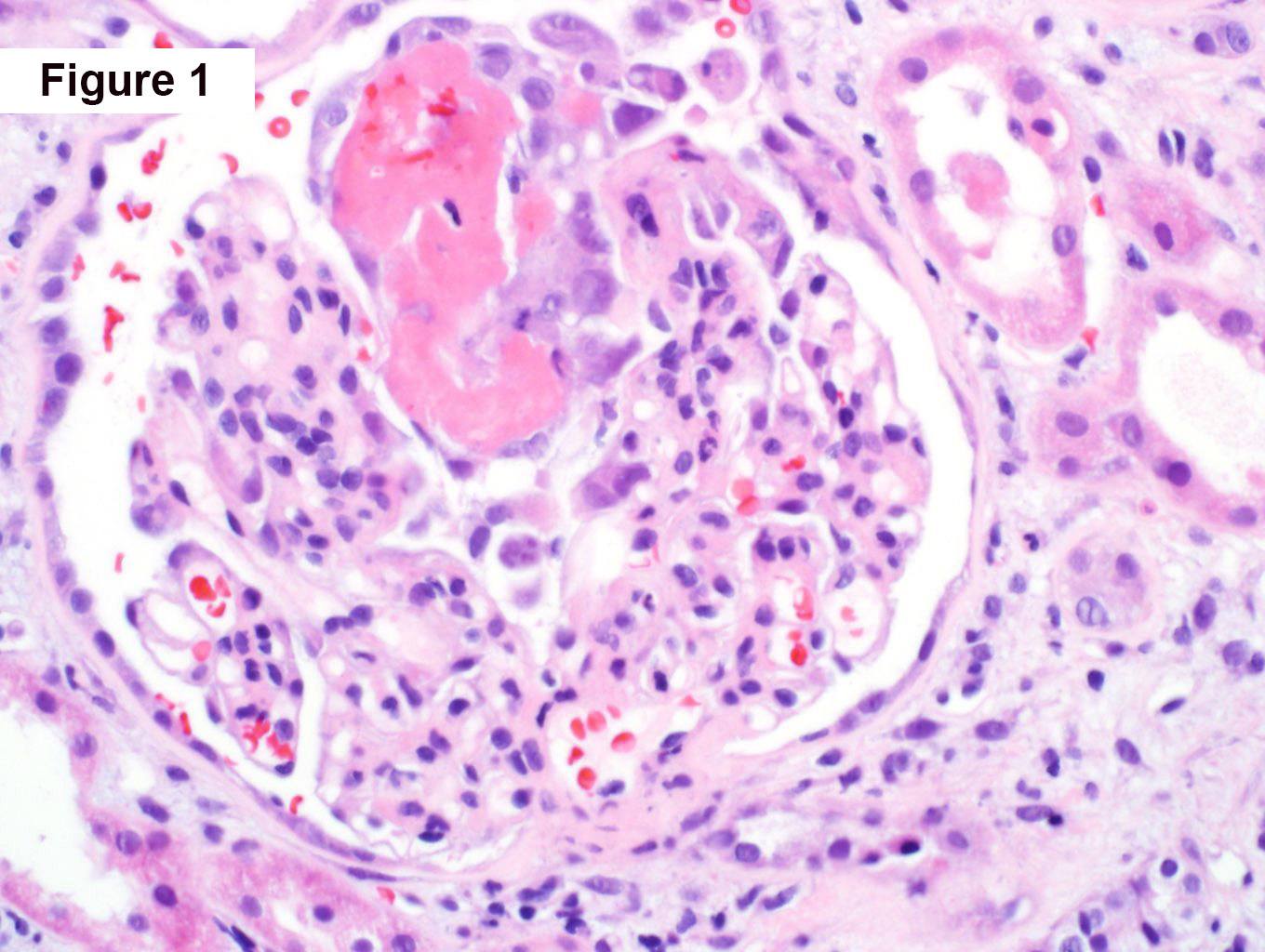
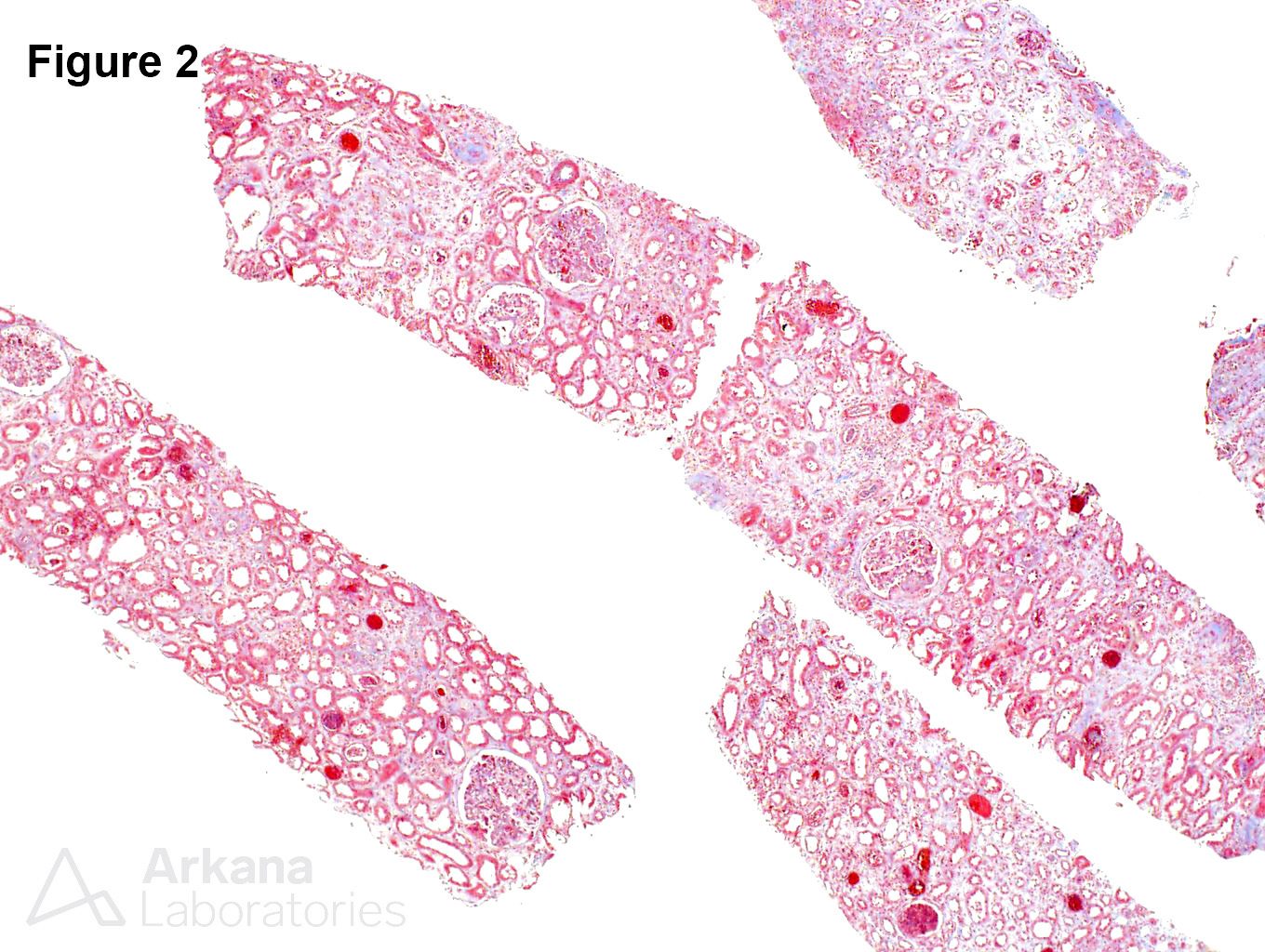
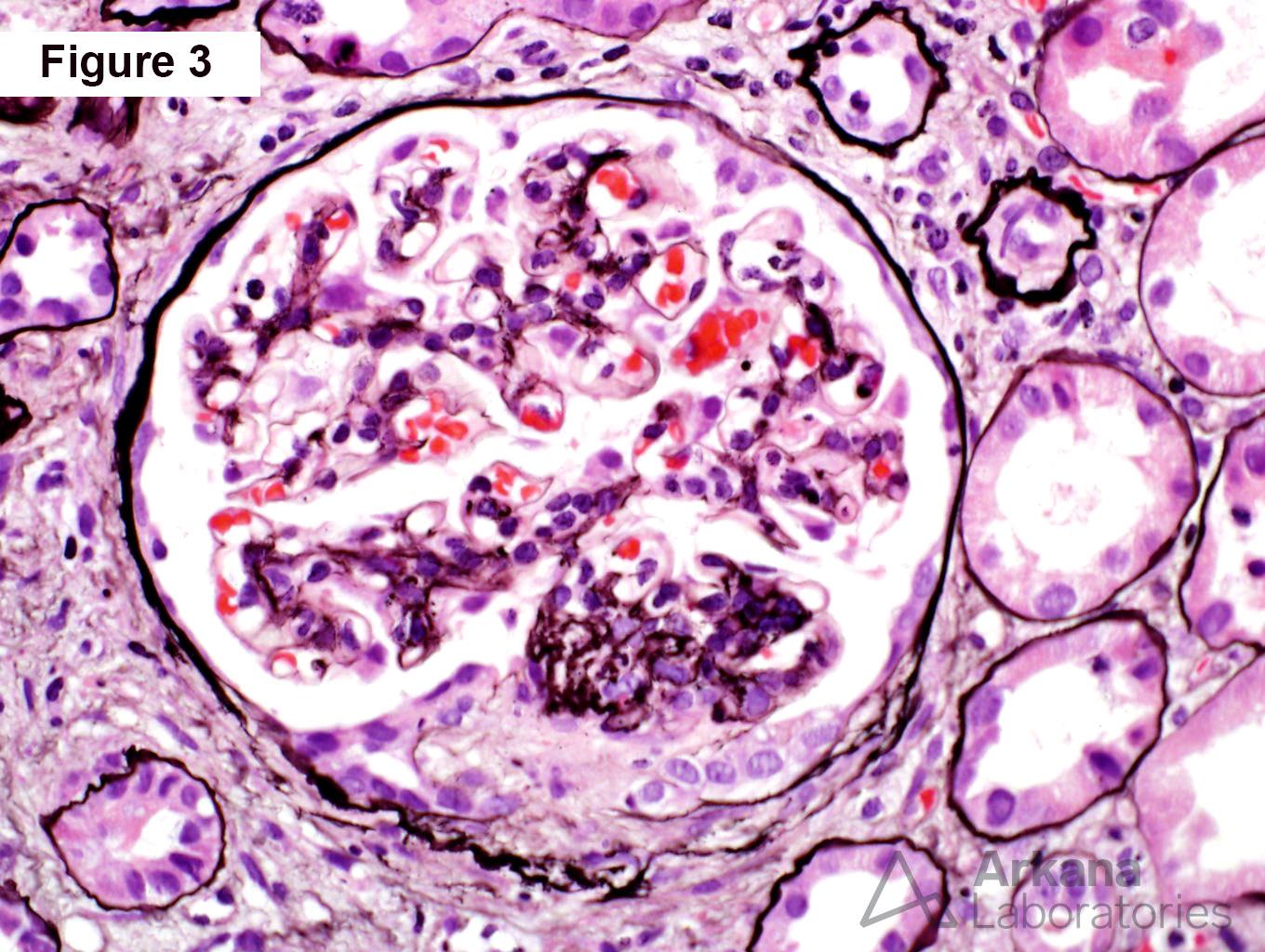
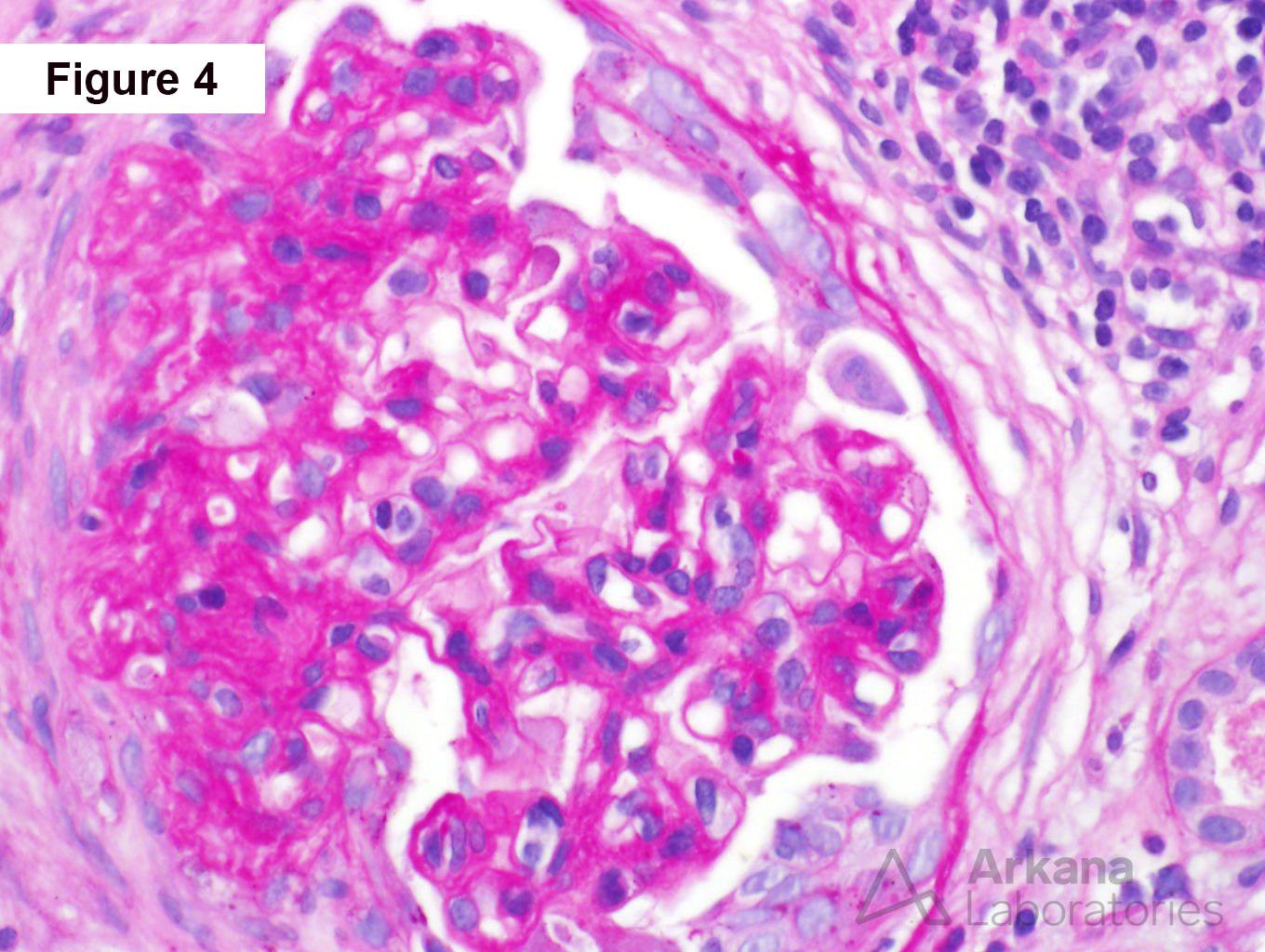
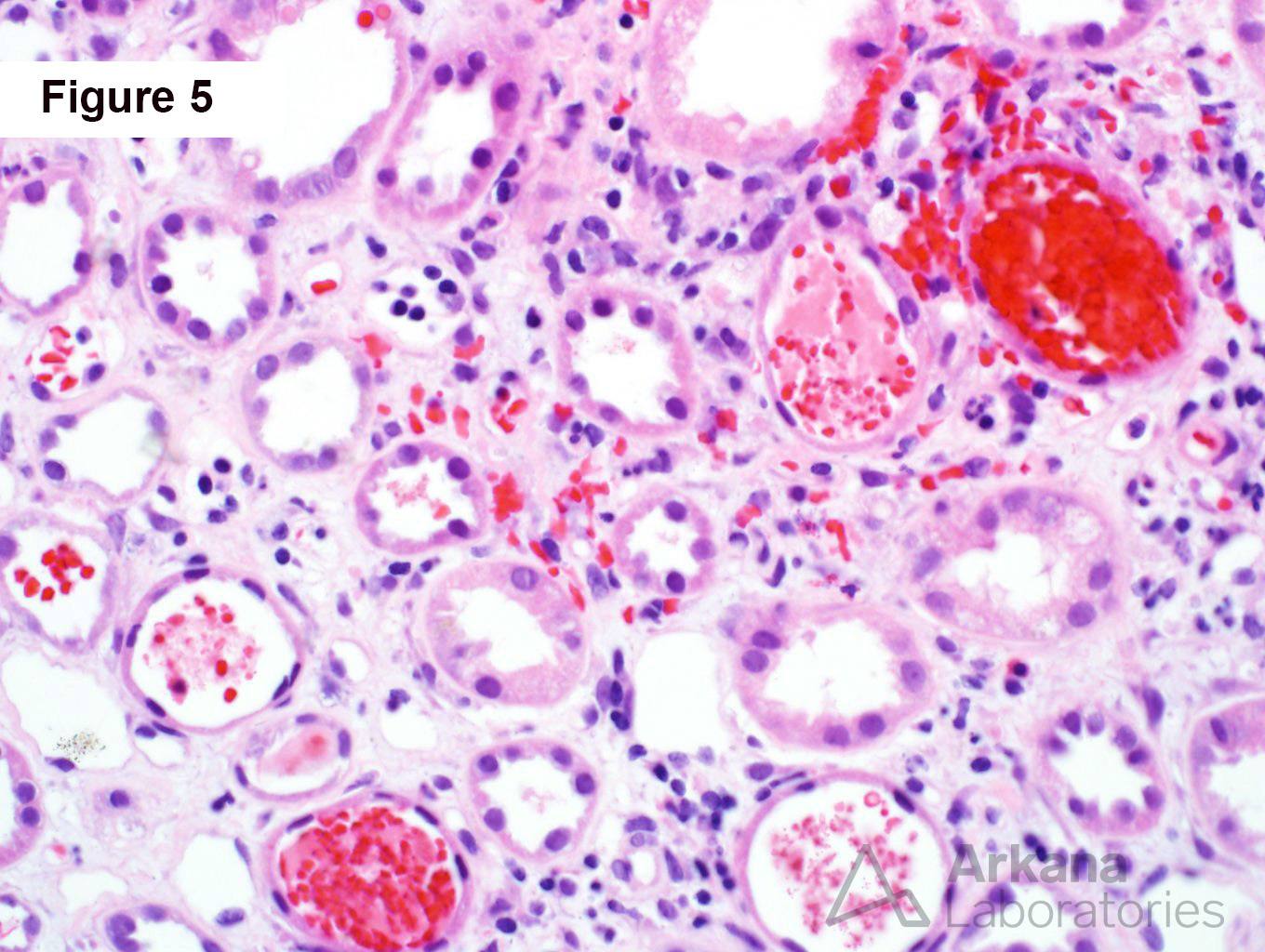
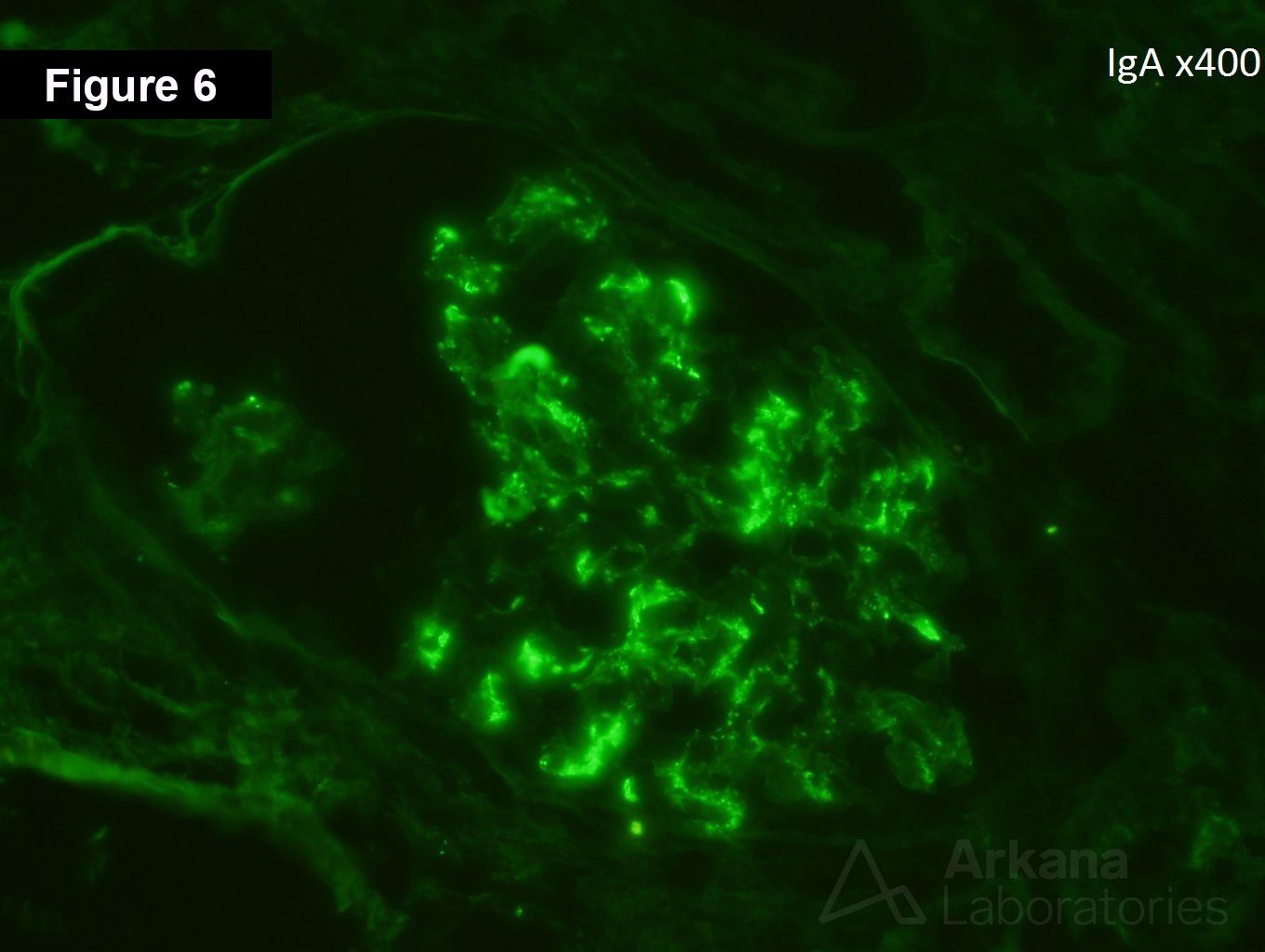
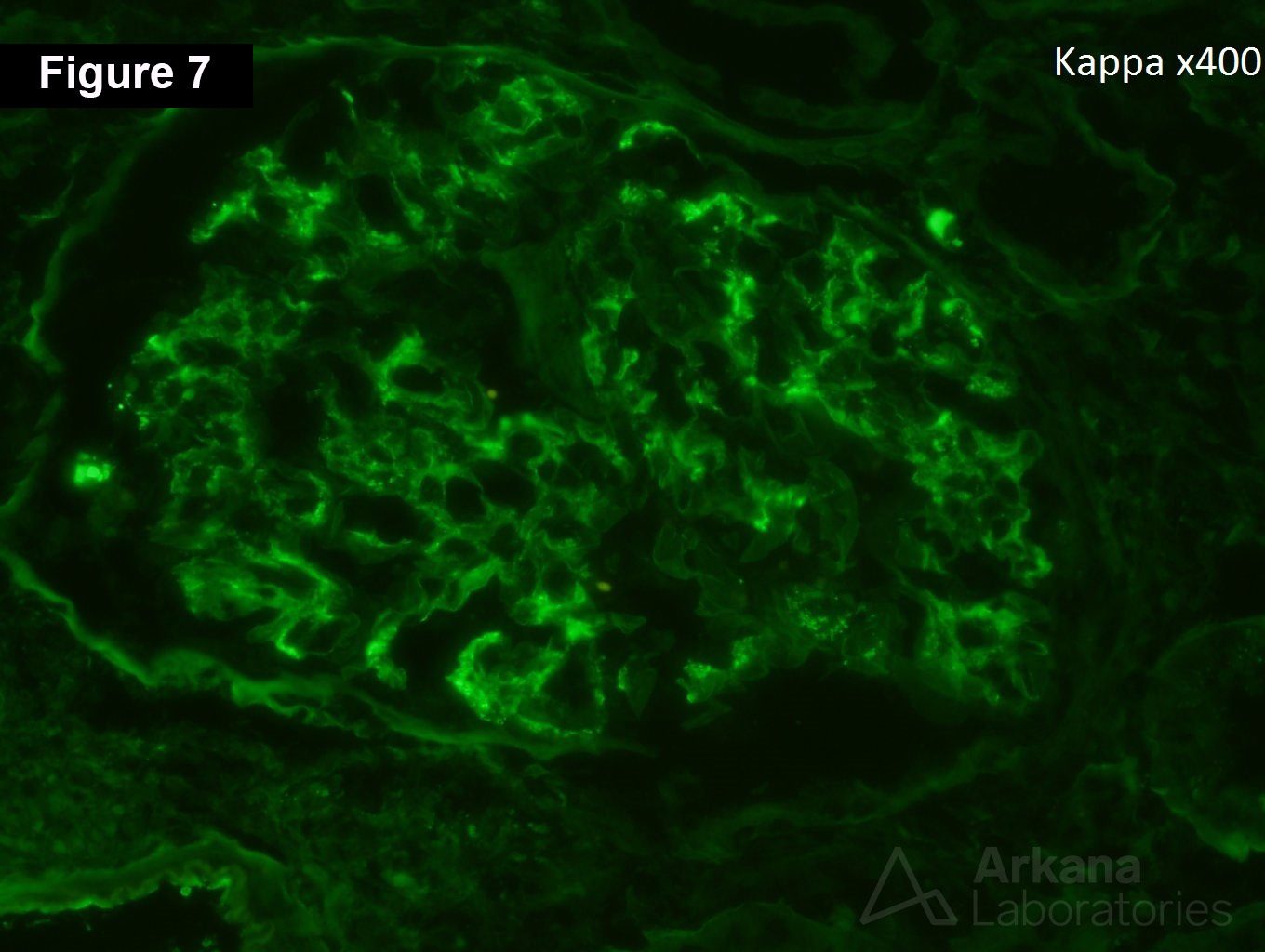
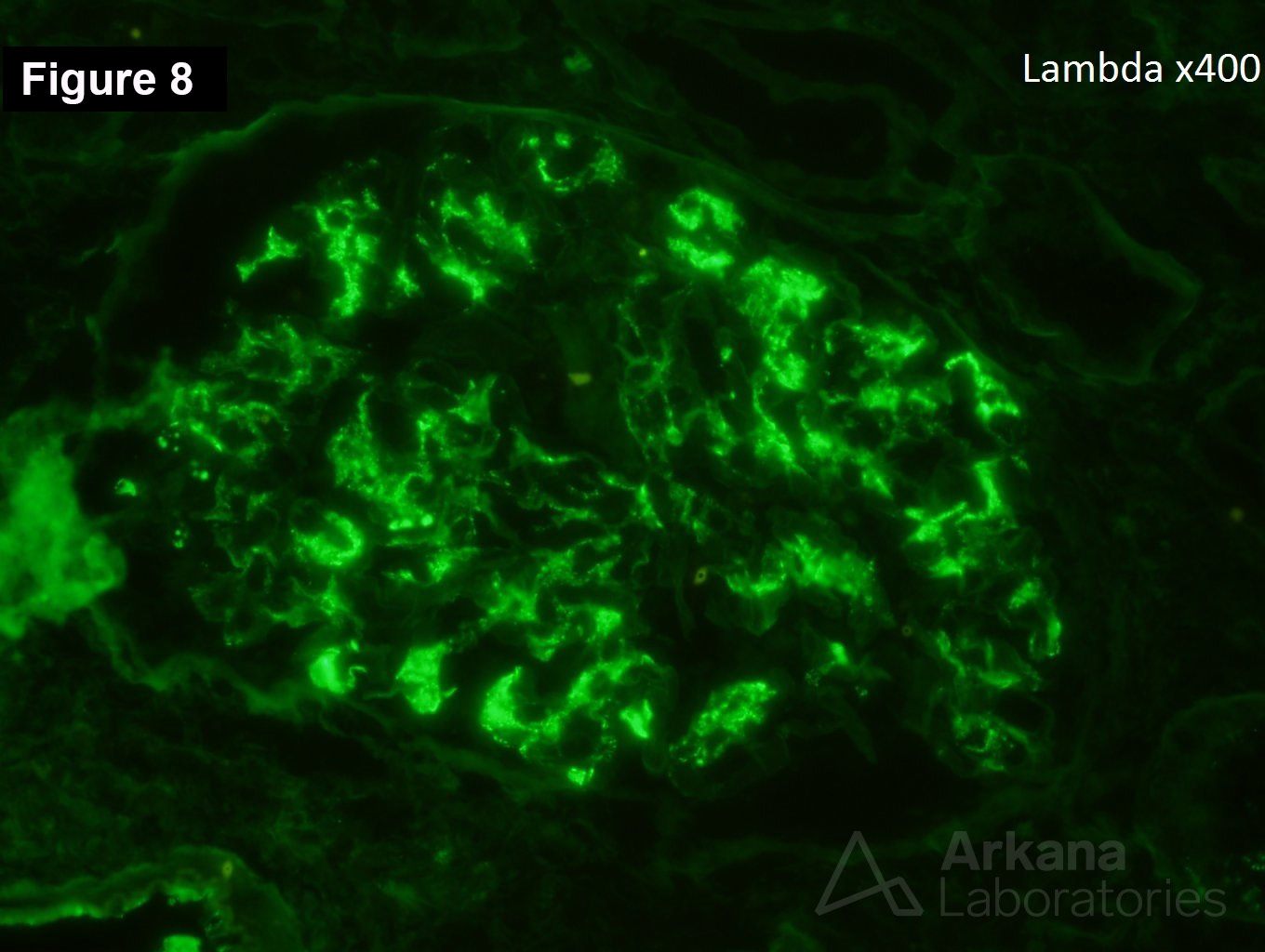
The patient is a 17-year-old white female who presents with 2.85 grams/24 hr proteinuria, microscopic hematuria, and a creatinine of 3.2 mg/dl. She was in her normal state of health and was incidentally found to have abnormal lab values and urinalysis at a routine sport’s physical. She reports that she had noticed a little more fatigue the last few months, but had blamed this on being busy at her job after school. Figure 1 shows focal fibrinoid necrosis. Figure 2 shows moderate tubular atrophy and interstitial fibrosis. Figures 3 & 4 show a segmental cellular crescent. Figure 5 shows several red blood cell casts. Figures 6, 7, & 8 shows IgA, kappa, and lambda, respectively.
The biopsy shows a focal crescentic IgA nephropathy. Earlier editions of the Oxford classification had not found crescents to be an independent predictor of poor renal outcomes in patients with IgA nephropathy. In a more recent meta-analysis of 3096 subjects, the presence of any cellular or fibrocellular crescent was independently associated with a worse prognosis in IgA nephropathy. The Oxford classification has now added a criteria for crescents: C0 (no crescents), C1 (less than 25% of glomeruli with crescents), and C2 (greater than 25% of glomeruli with crescents). Repeat renal biopsy studies in patients with IgA nephropathy have shown that crescents, fibrinoid necrosis, and endocapillary hypercellularity are potentially reversible with immunosuppressive therapy.
https://www.ncbi.nlm.nih.gov/pubmed/27612994
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.