What is your diagnosis?
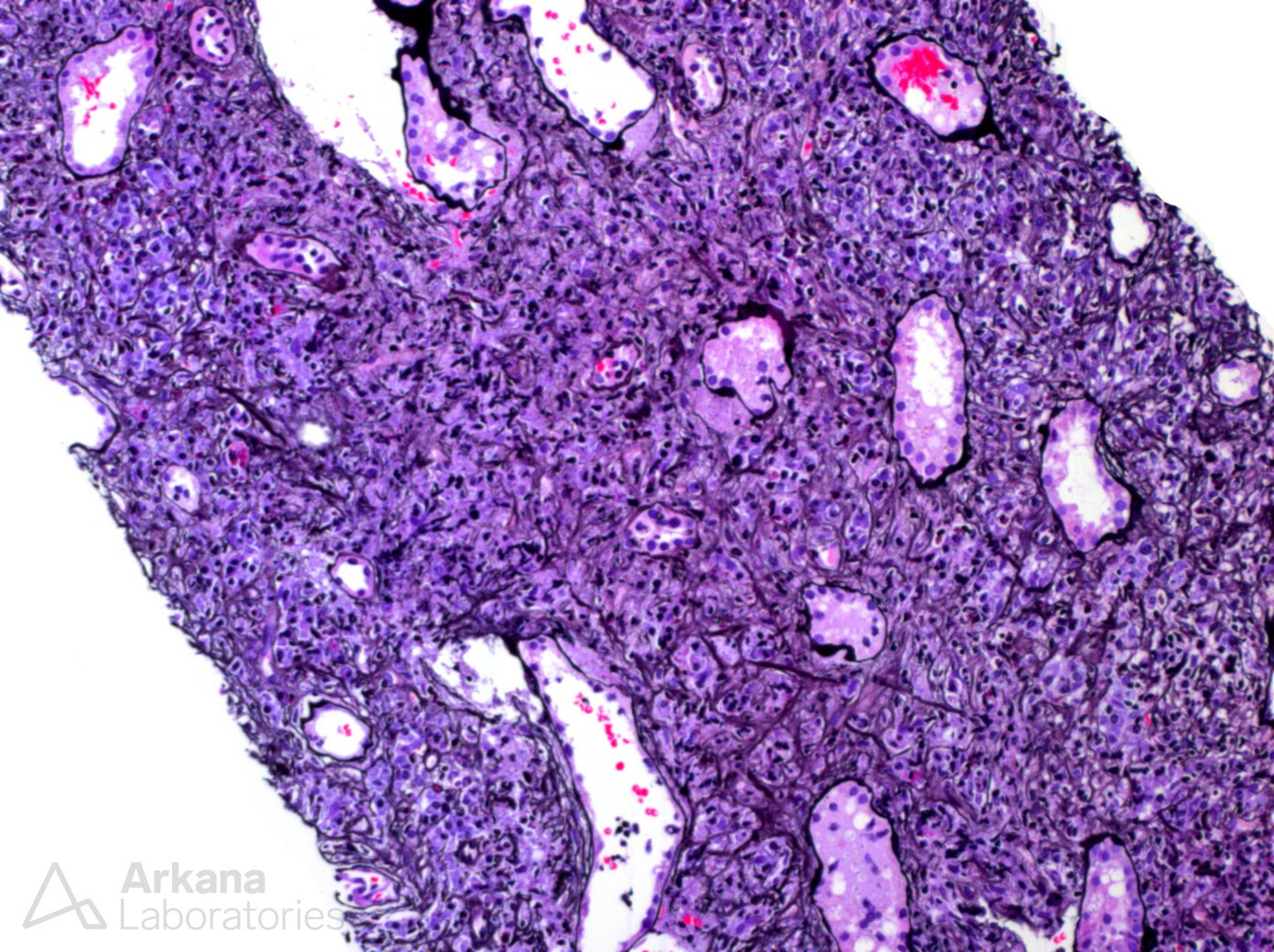
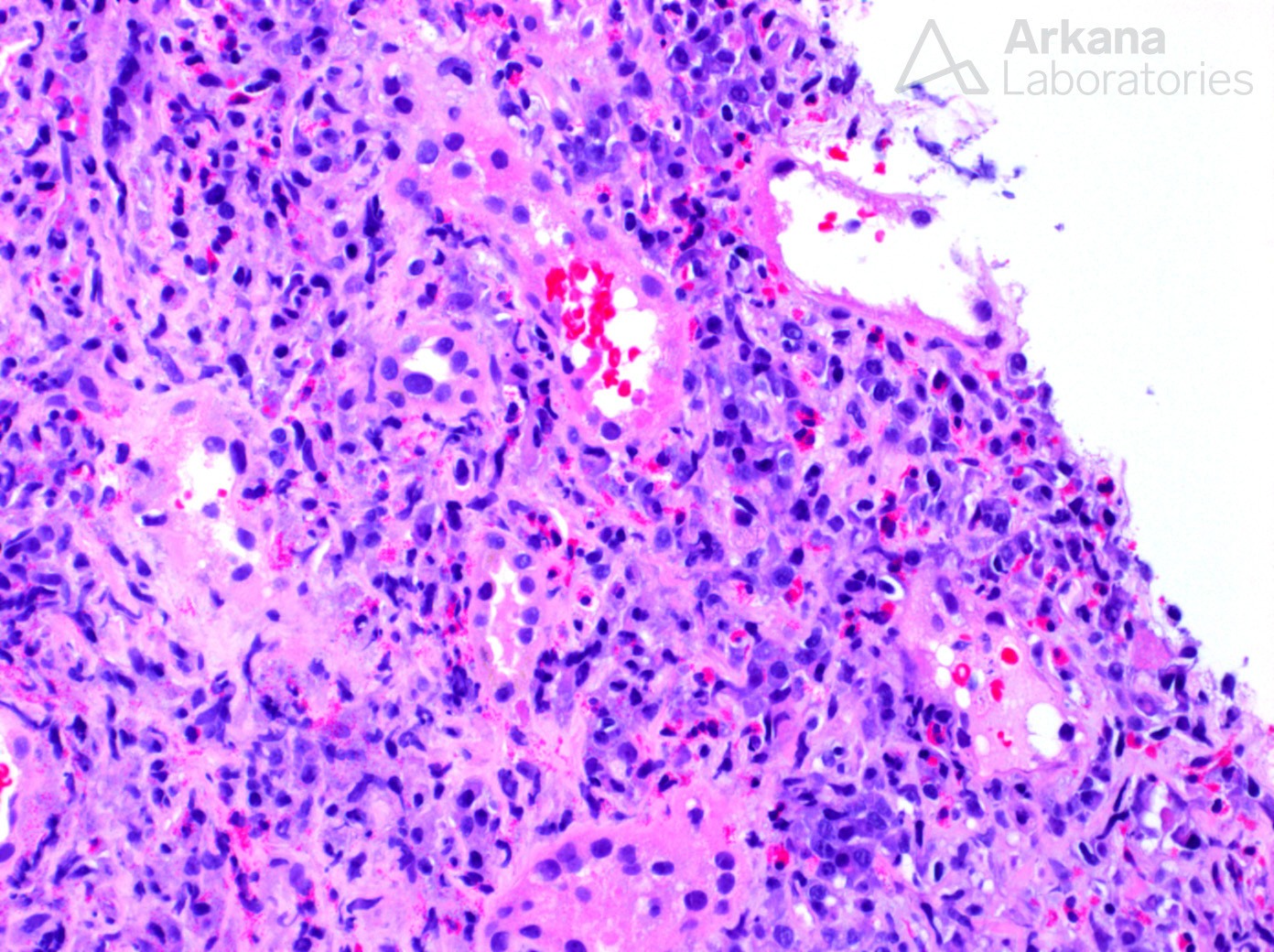
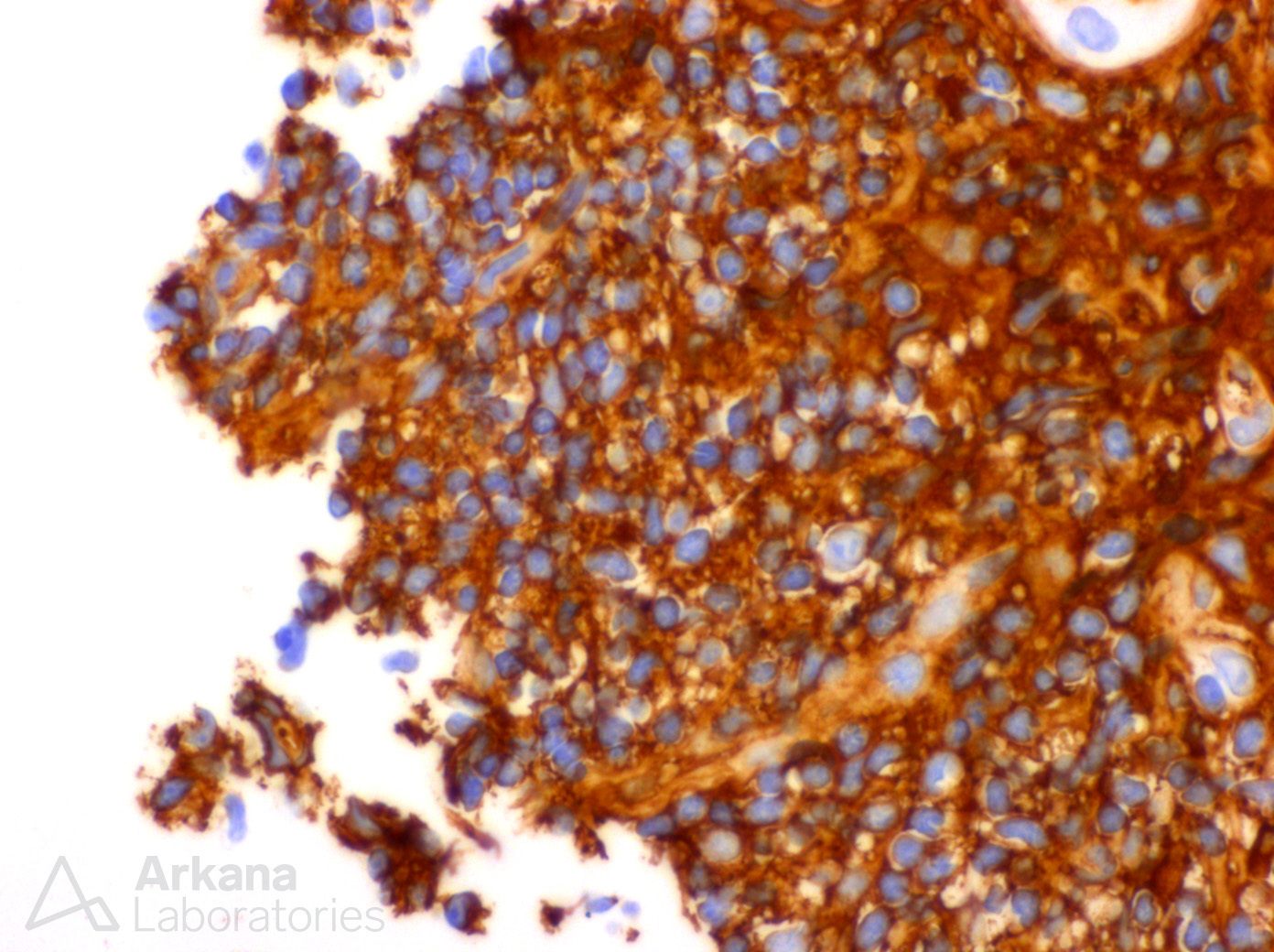
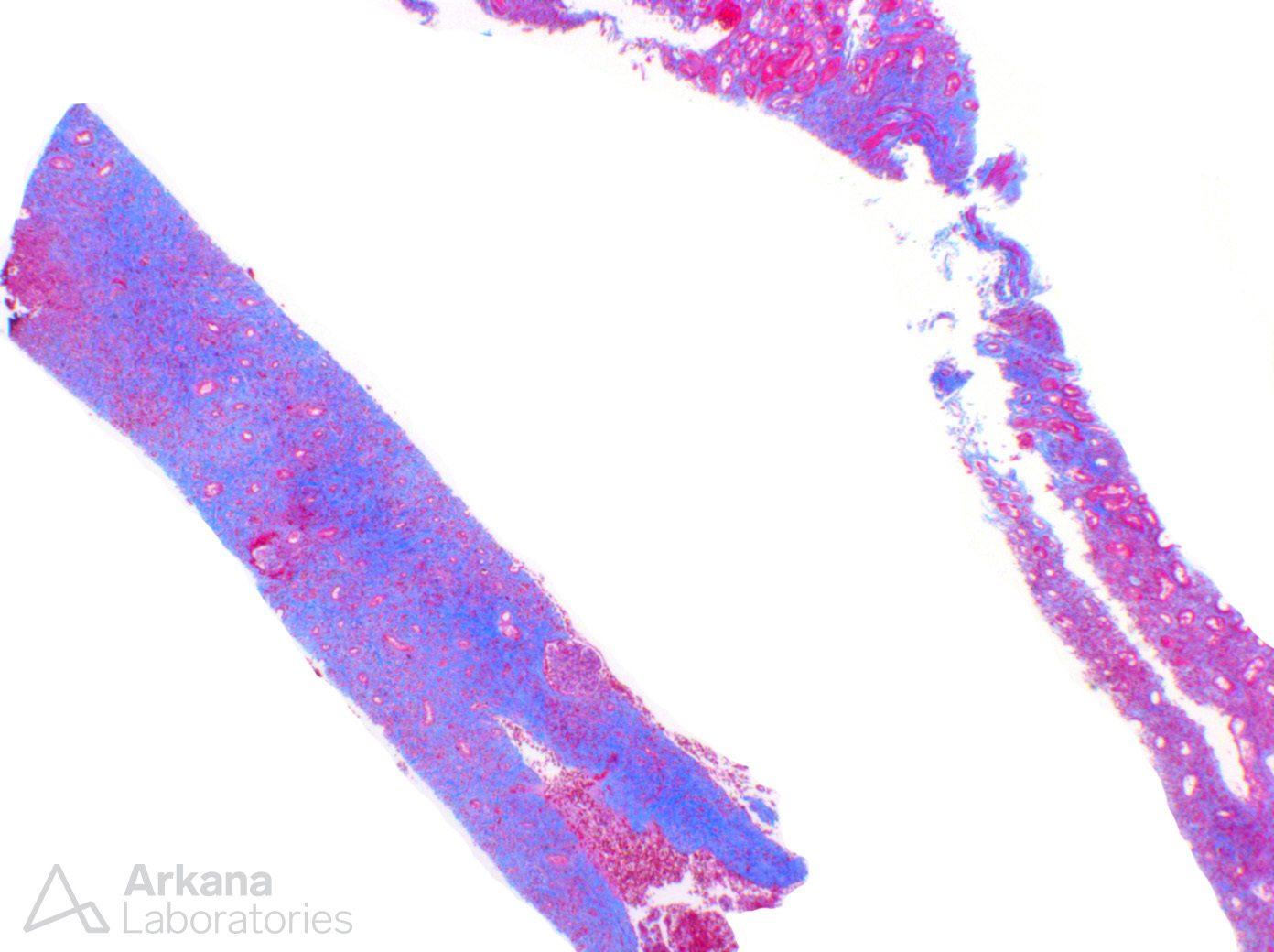
This biopsy shows a chronic, active tubulointerstitial nephritis with sharp demarcation between affected and non-affected tissue and a vague storiform pattern of fibrosis on silver stain. On H&E there is eosinophil and plasma cell rich inflammation and IgG4 staining (see image) which shows diffuse and extensive staining of the plasma cells and the background tissue. This pattern of injury is consistent with IgG4-related disease and merits further workup serologically and radiologically. Interestingly, the patient was initially diagnosed with an acute interstitial nephritis on biopsy in 2012 which was presumed to be secondary to NSAIDs use due to chronic, low grade abdominal pain of unknown etiology. He was treated with steroids and responded well. He presented again in 2016 with similar symptoms and had restarted NSAIDS as the pain had returned and was empirically treated with steroids and removal of NSAIDS which produced marked improvement. Unfortunately, this IgG4-related disease is eosinophil-rich and when predominantly acute (and potentially before widespread understanding of this relatively new disease), could be very difficult to distinguish from a drug/hypersensitivity reaction. In this case the patient had markedly elevated total serum IgG at his initial presentation in 2012 and in 2016 that reduced significantly after treatment both times and clinically they were unsure why he had increased IgG. Likely, this represents an increase in serum IgG4. And, as IgG4-related disease treated with steroids, the patient’s response was mistaken for resolution of drug/hypersensitivity reaction due to NSAIDs.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.