
Monday
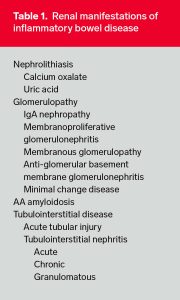
Extraintestinal manifestations of inflammatory bowel disease are common and involve nearly every organ system. Renal and urinary involvement has been reported to occur in 4% to 23% of inflammatory bowel disease patients manifested primarily as urinary calculi, fistulas, and ureteral obstruction.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4725142/
https://www.ncbi.nlm.nih.gov/pubmed/?term=pardi+AND+renal+and+urologic+complications
Parenchymal renal disease is rare but has been well documented in the form of case reports and small series describing glomerulonephritis, minimal change disease, secondary amyloidosis, and tubulointerstitial nephritis.
https://www.ncbi.nlm.nih.gov/pubmed/12722045
https://www.gastrojournal.org/article/S0016-5085(02)00276-7/fulltext
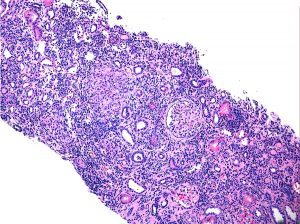
Renal biopsy is not frequently performed on patients with IBD, though it should be considered in patients presenting with renal insufficiency, proteinuria, or hematuria, particularly if other comorbid conditions are absent or renal insufficiency persists despite removal of nephrotoxic agents.
Tuesday
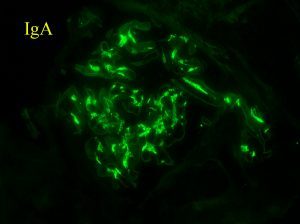
Glomerular involvement in IBD is rare, although several morphologic patterns of glomerular injury have been described:
- IgAN
- MPGN
- MCD
- Membranous
- Anti-GBM GN
- C3 GN
We published the largest case series of renal bx findings in IBD. IgAN was the most common dx (43% of all bx). The dx prevalence of IgAN was higher in IBD than in 33,630 non-IBD kidney bx during the same time period (24% versus 8%, P<0.001). https://www.ncbi.nlm.nih.gov/pubmed/24262508
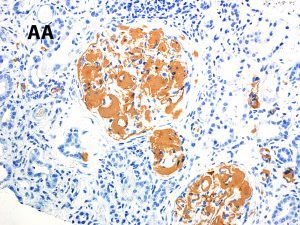
Amyloidosis A, so-called secondary amyloidosis, is a rare but serious complication of IBD. Studies have shown the prevalence of AA amyloidosis to be significantly higher in patients with Crohn disease than ulcerative colitis with a clear predilection in men.
Amyloidosis A is also more commonly presents is those with long-standing disease, in particular those with fistulizing-stenotic forms, suppurative complications, and ileocolonic involvement. https://www.ncbi.nlm.nih.gov/pubmed/?term=tosca+cuquerella+AND+amyloidosis
Wednesday
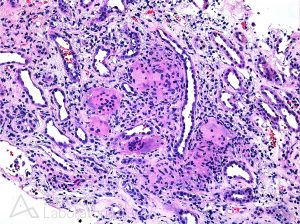
Acute tubular injury and tubulointerstitial nephritis (TIN) have been reported as both an extraintestinal manifestation of IBD as well as a complication of IBD-related therapy. https://www.ncbi.nlm.nih.gov/pubmed/11472315
There have been several case reports of both acute and chronic (TIN) occurring in patients with both Crohn disease and ulcerative colitis, particularly in the setting of 5-ASA drug therapy and its derivatives.
In our series, TIN was the second most common finding in kidney biopsies of IBD patients after IgA nephropathy (19%). This included cases of both acute and chronic TIN and it was more frequently seen in patients with ulcerative colitis (69%). https://www.ncbi.nlm.nih.gov/pubmed/15007714
While acute and chronic TIN is commonly associated with IBD-related therapy/drug exposure, there have been several reports of TIN presenting concurrently with IBD diagnosis in drug-naïve patients.
Interestingly, granulomatous TIN has been reported in drug-naïve patients with Crohn disease. This suggests TIN may actually represent a true extraintestinal manifestation of IBD in certain patients. https://www.ncbi.nlm.nih.gov/pubmed/24377821
Thursday
Although the frequency of renal involvement in pediatric IBD is not well described, there have been several reports of nephrolithiasis, GN (particularly IgAN), TIN, and rarely AA amyloidosis.
https://www.ncbi.nlm.nih.gov/pubmed/15971070
https://www.ncbi.nlm.nih.gov/pubmed/23782372
A recent literature review of the pediatric IBD population with renal manifestations found a strong predilection in boys (72%) and those with Crohn disease (80%). https://www.ncbi.nlm.nih.gov/pubmed/26223844
The most common renal manifestations in the pediatric IBD population with renal manifestations was nephrolithiasis (58%) followed by TIN (30%), which was present in two-thirds of UC pts. https://www.ncbi.nlm.nih.gov/pubmed/26223844
Friday
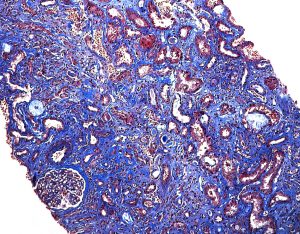
Inflammatory bowel disease (IBD) is a condition characterized by chronic inflammation of the gastrointestinal tract with the two most common types Crohn disease and ulcerative colitis. While renal and urinary involvement in IBD is not uncommon, renal parenchymal disease is rare and most commonly affects the glomerular and tubulointerstitial compartments.
The most common findings on renal biopsy of IBD patients are IgA nephropathy and tubulointerstitial nephritis, and this occurrence may represent a common pathogenic mechanism. Although several cases of tubulointerstitial nephritis have been related to drug exposure, there is increasing evidence that this finding may also represent a true extraintestinal manifestation of disease.
The overall morbidity of IBD-related renal manifestations is significant, and there is often only a short window of injury reversibility. This, along with an often subtle clinical presentation, requires a high index of suspicion and likely routine monitoring of renal function, particularly in the elderly and those with co-morbidities. There are currently no established guidelines for the optimal screening and monitoring of renal function in IBD patients. However, there appears to be general consensus that renal function should be assessed prior to initiation of drug therapy, with ongoing monitoring of renal function every 3 months to 6 months the first year, followed by annual to semiannual monitoring thereafter.
https://www.ncbi.nlm.nih.gov/pubmed/?term=ambruzs+AND+renal+manifestations+of+inflammatory
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.