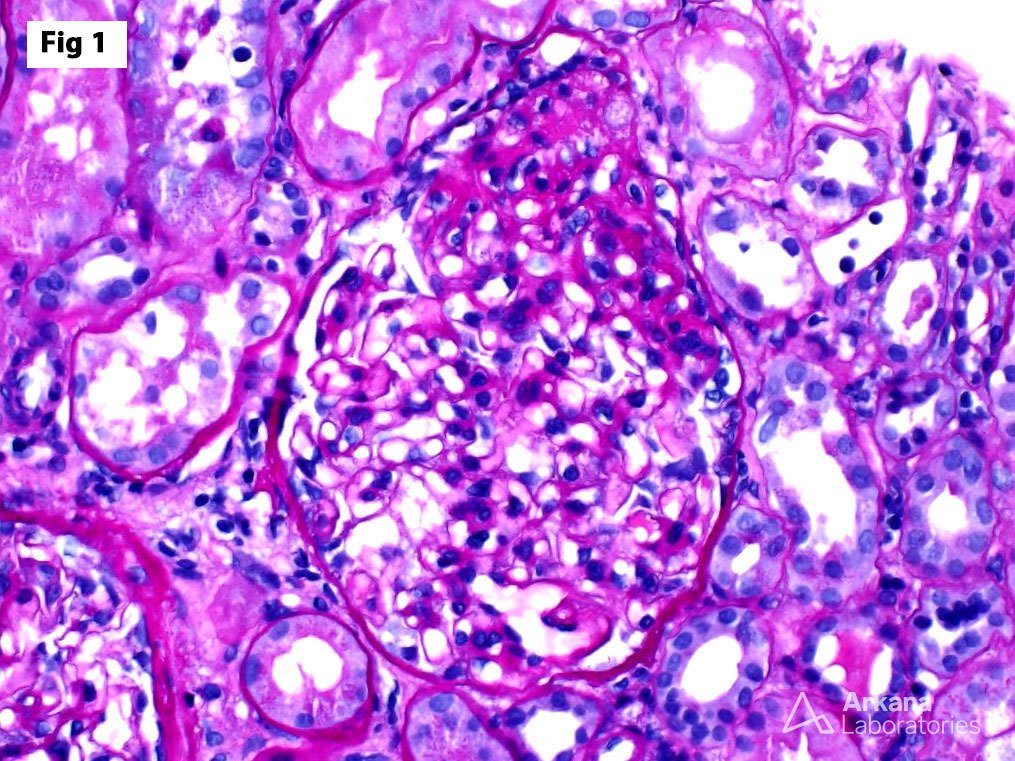
This biopsy is from a 35-year-old male with no significant medical history, who presents with sudden onset nephrotic syndrome. At presentation, the UPCR was 8.2 g/g and the serum albumin was 1.1 g/dl. Renal function was preserved (SCr 1.1 mg/dl). The biopsy shows frequent areas of segmental glomerulosclerosis (FSGS), associated with endocapillary foam cells and epithelial cell capping, predominantly involving the takeoff point of the proximal tubule (fig 1). Focally, the areas of segmental sclerosis herniate into the proximal tubule. Immunofluorescence is completely negative within the glomeruli, and electron microscopy (fig 2) shows diffuse epithelial foot process effacement. The findings are indicative of a primary podocytopathy as the cause of this patient’s nephrotic syndrome. According to the Columbia classification, this lesion meets criteria for a tip variant of FSGS. Focal segmental glomerulosclerosis is a morphologic pattern of glomerular injury which may arise as a consequence of a wide variety of glomerular disorders. It may be indicative of a primary podocyte disease or may represent an adaptive response to excess demand on glomerular function. The tip variant of FSGS usually represents a primary podocytopathy, has the best prognosis among the various forms of FSGS, the highest responsivity to steroid therapy and the lowest risk of progression.

Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.