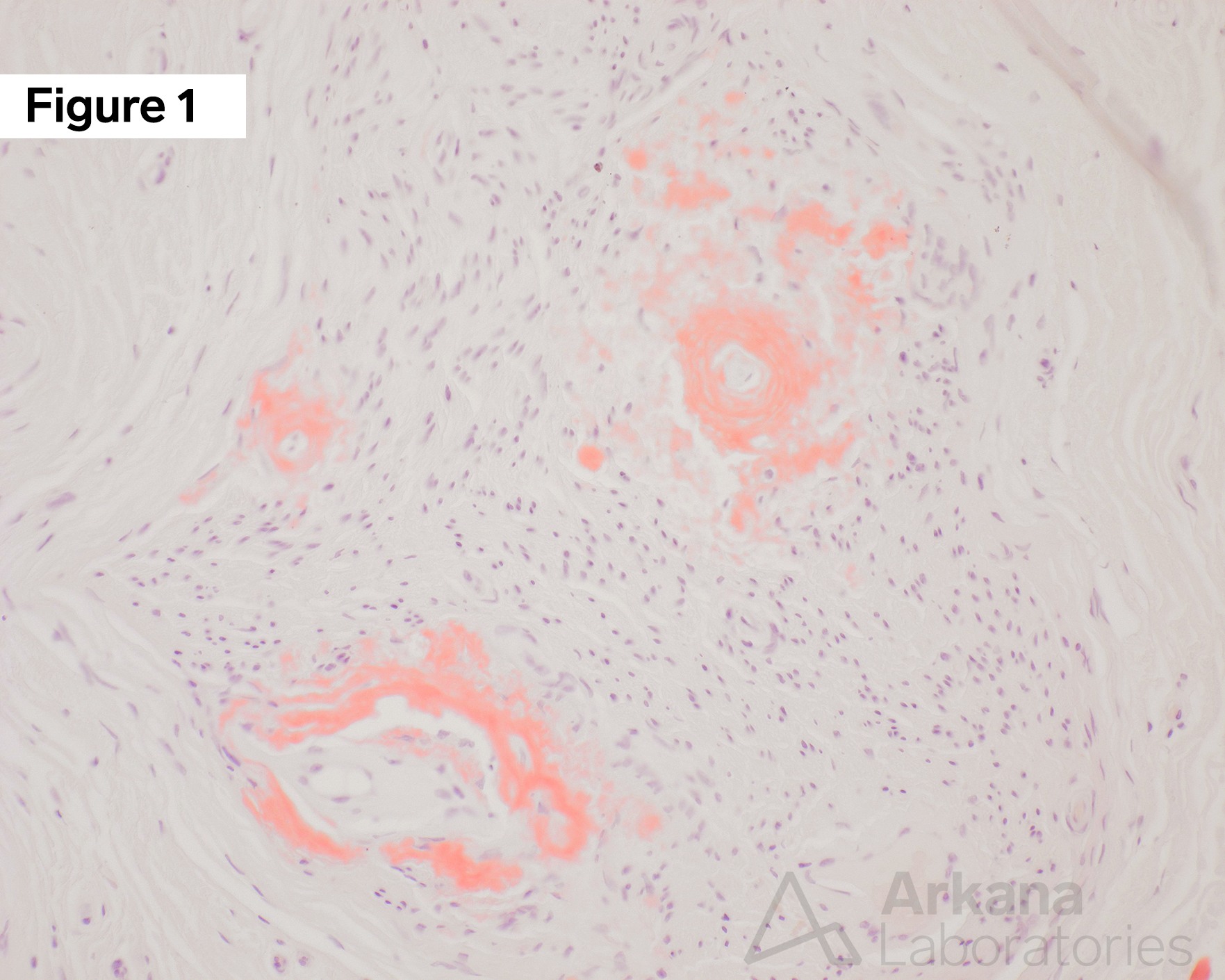
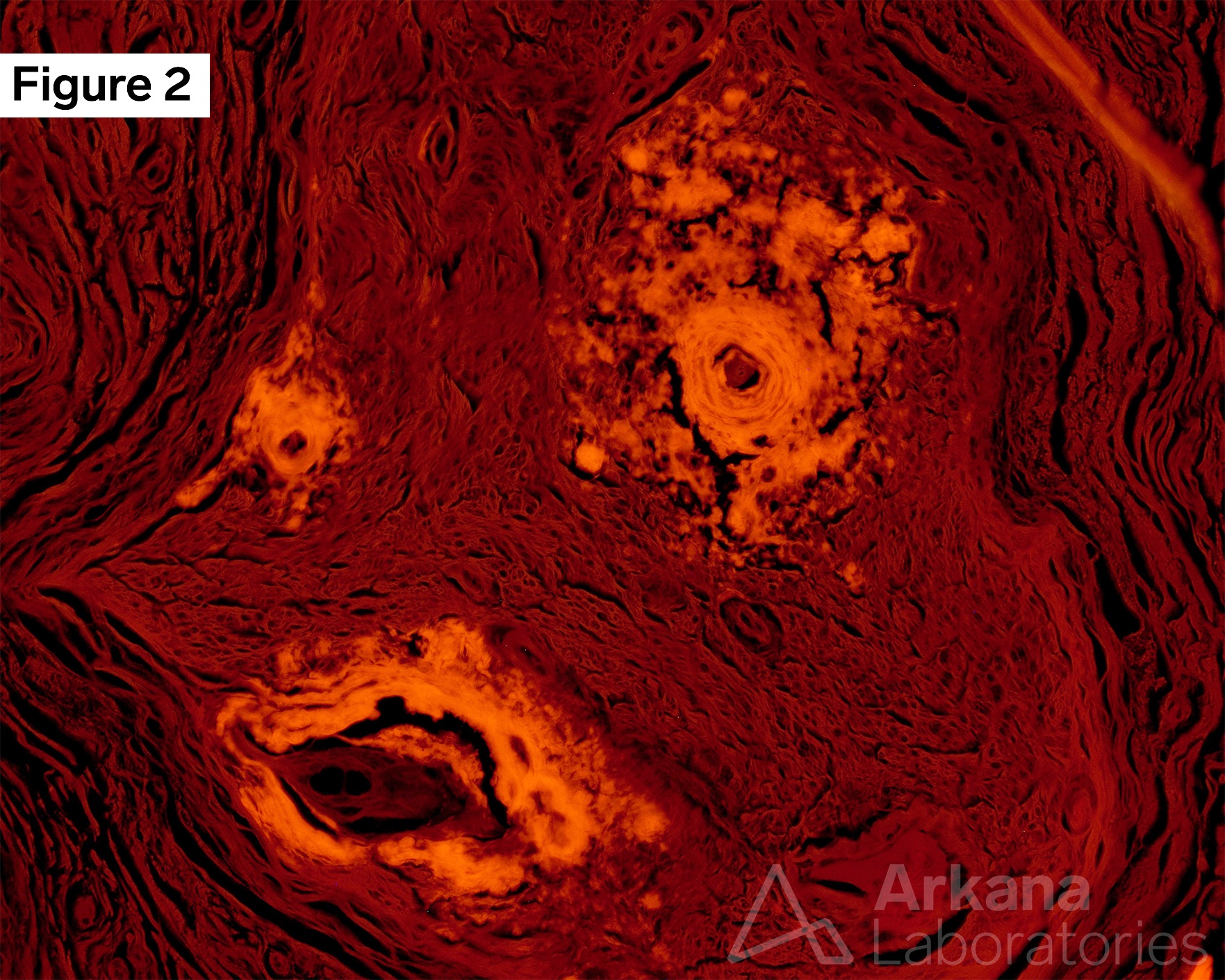
Elderly female with amyloid neuropathy of the sural nerve. Cross-sections of the left sural nerve prepared from formalin-fixed paraffin-embedded (FFPE) tissue stained with Congo red show dense salmon-orange material (i.e. congophilic) predominantly around endoneurial blood vessels (Figure 1), as well as a few small accumulations within nerve fascicles, diagnostic of amyloid deposition. The material shows apple-green birefringence with compensated polarized light microscopy (not shown), and also shows an intense bright red glow (Figure 2) against a dull background under UV light fluorescence microscopy with a Texas red excitation filter (i.e. rhodamine optics). Co-localization to the same nerve fascicle, original magnifications: A. FFPE, Congo Red, Routine Light Microscopy, 200x; and B. FFPE, Congo Red, UV Fluorescence Microscopy with TR Filter, 200x.
The patient is an elderly female (8th decade) who presents with a complaint of numbness in her hands and feet. Her symptoms have been progressive, and have resulted in recent falls. While she has many chronic co-morbidities, she is not a diabetic. She does not have any liver disease, and her SPEP studies are normal. No family history of a primary intrinsic muscle and/or nerve disorder is reported. Due to paresthesias of uncertain etiology, the decision was made to pursue peripheral nerve biopsy of the left sural nerve. Neuropathologic examination of the nerve revealed Congophilic material diagnostic of amyloid; however, attempt to subtype the amyloid failed. Using the images above, alteration in which of the following genes may lead to hereditary/familial amyloid polyneuropathy?
A. N-MYC
B. ATRX
C. TTR
D. NOTCH3
Answer: TTR
The images show amyloid deposition in a peripheral, which did not further subtype, such findings may be seen in Transthyretin-related familial amyloid polyneuropathy (TTR-FAP). See references below, text directly quoted from Çakar A, et al. 2019.
TTR-FAP is a life-threatening disease caused by the accumulation of amyloidogenic transthyretin (TTR) protein in tissues.
Mutations in the TTR gene (correct answer choice C) destabilize TTR protein to misfold from its native tetramer form to amyloidogenic monomer form.
In endemic countries, TTR-FAP presents with length-dependent small fiber neuropathy, however, in non-endemic countries clinical features can be highly variable.
Genetic testing for TTR gene is mandatory for the diagnosis, and mass spectrometry-bases proteomic analysis may also be helpful to evaluate these patients.
Why were the other answers wrong?
N-MYC (answer choice A) may be amplified or otherwise altered in cancers, including pediatric malignancies of retinoblastoma and neuroblastoma.
In the neuropathology realm, ATRX (answer choice B) mutations are associated with brain tumors (i.e. IDH-mutant astrocytomas).
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is an important cause of stroke in young adults caused by mutations in the NOTCH3 gene (answer choice D), which encodes a transmembrane receptor expressed in vascular smooth muscle cells.
References
Asiri MMH, Engelsman S, Eijkelkamp N, Höppener JWM. Amyloid proteins and peripheral neuropathy. Cells. 2020 Jun 26;9(6):1553. PMID: 32604774.
Çakar A, Durmuş-Tekçe H, Parman Y. Familial Amyloid Polyneuropathy. Noro Psikiyatr Ars. 2019 May 6;56(2):150-156. PMID: 31223250.
Klein CJ, Vrana JA, Theis JD, Dyck PJ, et al. Mass spectrometric-based proteomic analysis of amyloid neuropathy type in nerve tissue. Arch Neurol. 2011 Feb;68(2):195-9. PMID: 20937937.
Picken MM. The pathology of amyloidosis in classification: a review. Acta Haematol. 2020;143(4):322-334. PMID: 32392555.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.