An elderly but previously healthy patient presents with weakness and fatigue and was found to have a creatinine of 3.0 mg/dl. His baseline Cr was 1.2 mg/dl four months prior. No history of diabetes or hypertension. Biopsy performed for kidney injury, acute versus chronic.
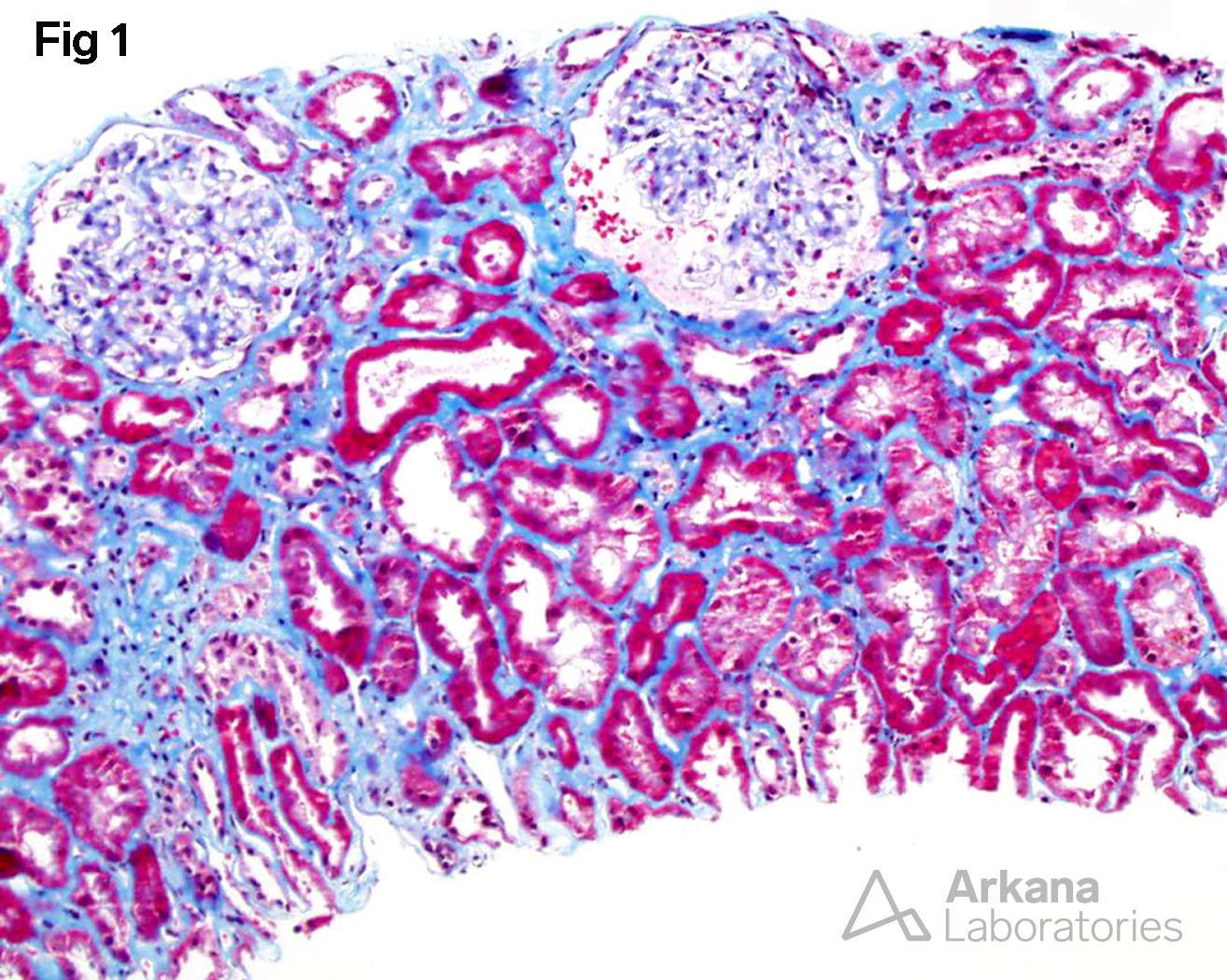
Tubular Injury, interstitial fibrosis, and intact glomeruli.
1. Tubular Injury, interstitial fibrosis, and intact glomeruli
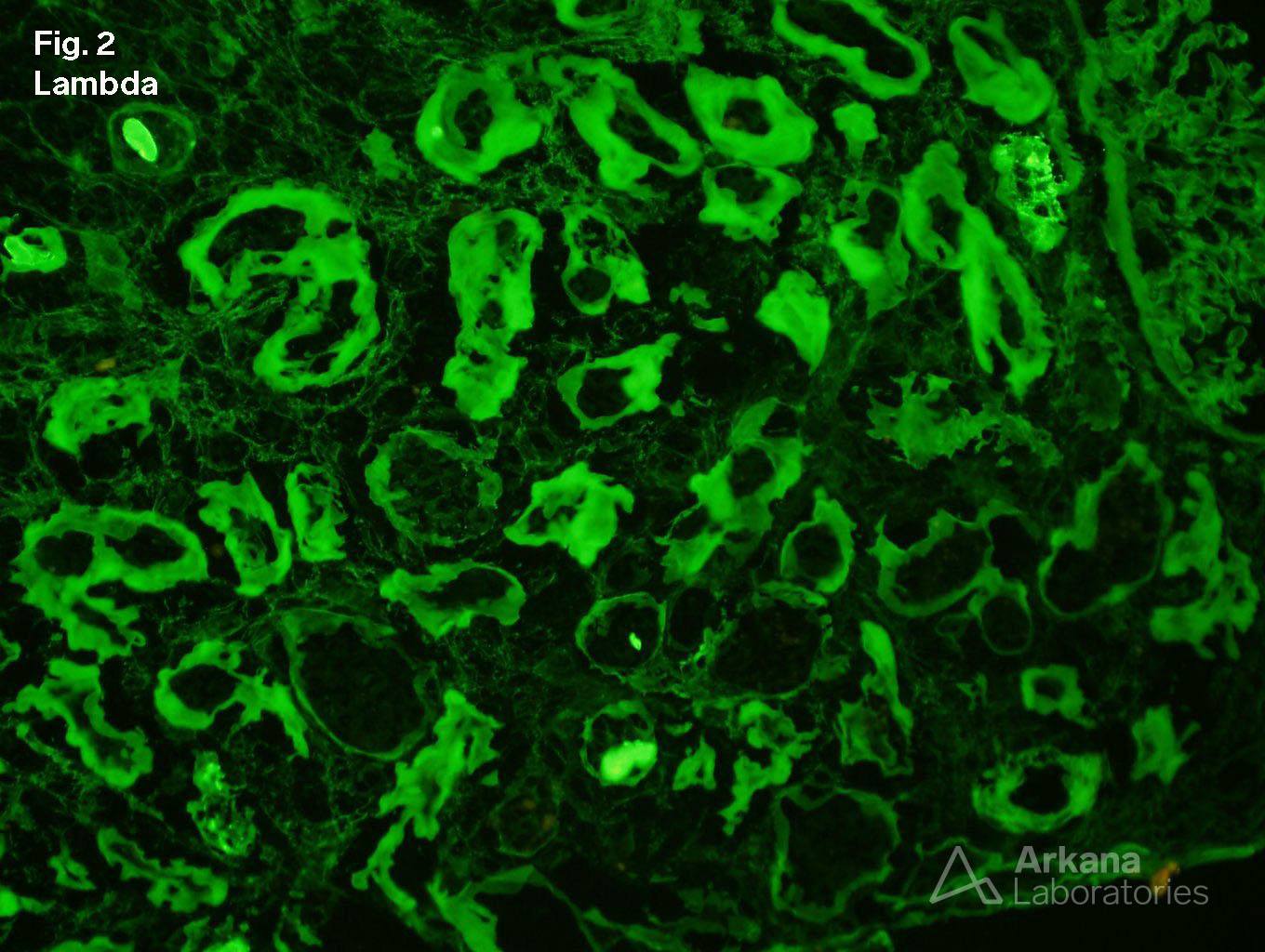
2. Linear staining for lambda light chains along tubular basement membranes
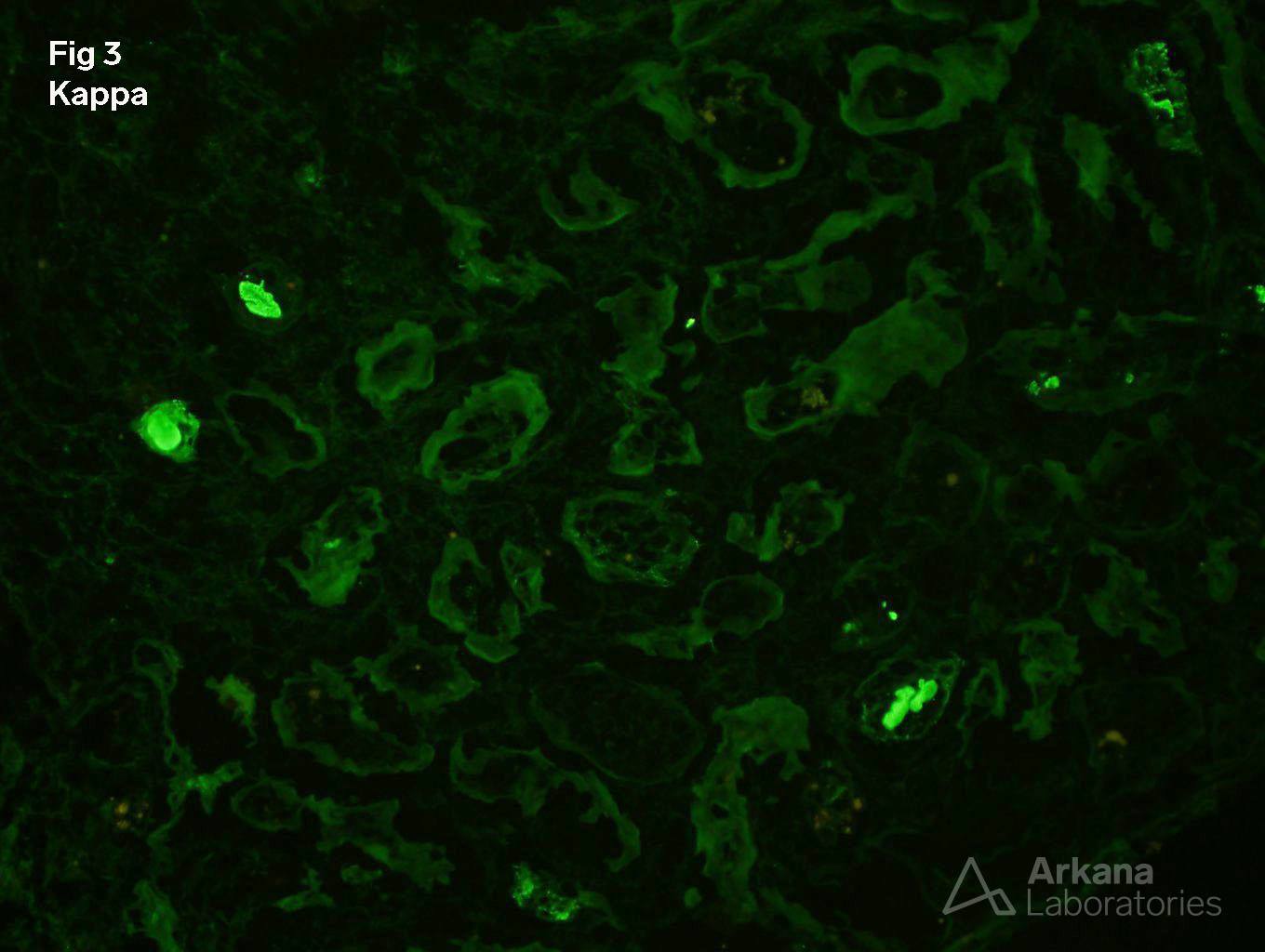
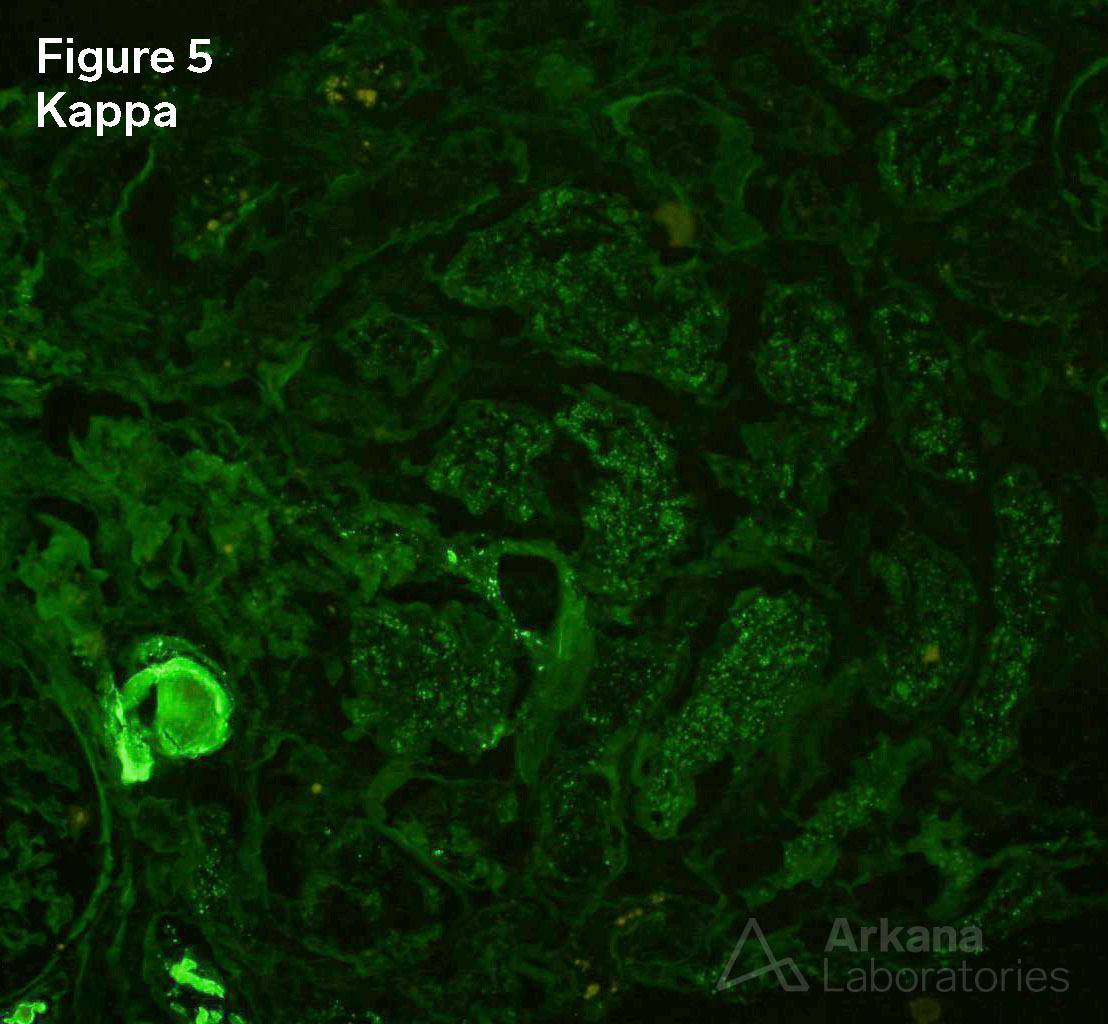
3. Negative staining for kappa light chains along tubular basement membranes
4. Positive Lambda staining in tubular droplets
5. Negative Kappa staining in tubular droplets
Electron microscopy was negative for tubular basement membrane deposits and negative for tubular epithelial cell crystalline inclusions.
Diagnosis:
Light Chain Proximal Tubulopathy, Lambda Light Chain Type
Immunofluorescence Features Consistent with Light Chain Deposition Disease, Lambda Light Chain Type
Acute Tubular Injury
Interstitial Fibrosis, Mild
Arteriosclerosis, Severe
Follow Up:
SPEP showed an abnormal IgG/Lambda band. Bone marrow biopsy contained >20% plasma cells. Renal biopsy changes are considered characteristic of a monoclonal gammopathy of renal significance (MGRS) and treatment was begun.
Discussion:
Light Chain Deposition Disease (LCDD), also called Monoclonal Immunoglobulin Deposition Disease (MIDD), is characterized by thickened tubular basement membranes (TBMs) and nodular glomerulosclerosis by light microscopy (LM). Immunofluorescence microscopy (IF) shows the monoclonal nature of the disease with linear deposits of either kappa or lambda light chains along the TBMs, the glomerular basement membranes and within the mesangium. Electron microscopy (EM) demonstrates the light chain deposition as powdery deposits along TBMs, GBMs and in the expanded mesangial areas. These diagnostic criteria are based on ‘tip of the iceberg’ cases. That is cases that are well along in their course with the classic pattern of LCDD. But what do biopsies from patients with new onset disease look like? This patient, fortunately, appears to have presented very early in the course of multiple myeloma. The renal biopsy shows none of the classic LM features of LCDD. In fact, the only changes on LM are arteriosclerosis and acute tubular injury consistent with tubular injury due to the tubular toxicity of light chains. By EM, there are essentially no changes. Particularly no TBM deposits are seen despite an extensive search. Still, the characteristic IF pattern is present and strongly suggests LCDD. This, along with the presence of light chain proximal tubulopathy, led to a rapid workup and diagnosis of multiple myeloma with end-organ damage.
References:
1. Gokden N, Barlogie B, Liapis H: Morphologic heterogeneity of renal light-chain deposition disease. Ultrastruct Pathol 2008, 32:17-24. https://www.ncbi.nlm.nih.gov/pubmed/18300034
2. Larsen CP, Bell JM, Harris AA, Messias NC, Wang YH, Walker PD: The morphologic spectrum and clinical significance of light chain proximal tubulopathy with and without crystal formation. Mod Pathol 2011, 24:1462-9. https://www.nature.com/articles/modpathol2011104?foxtrotcallback=true
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.