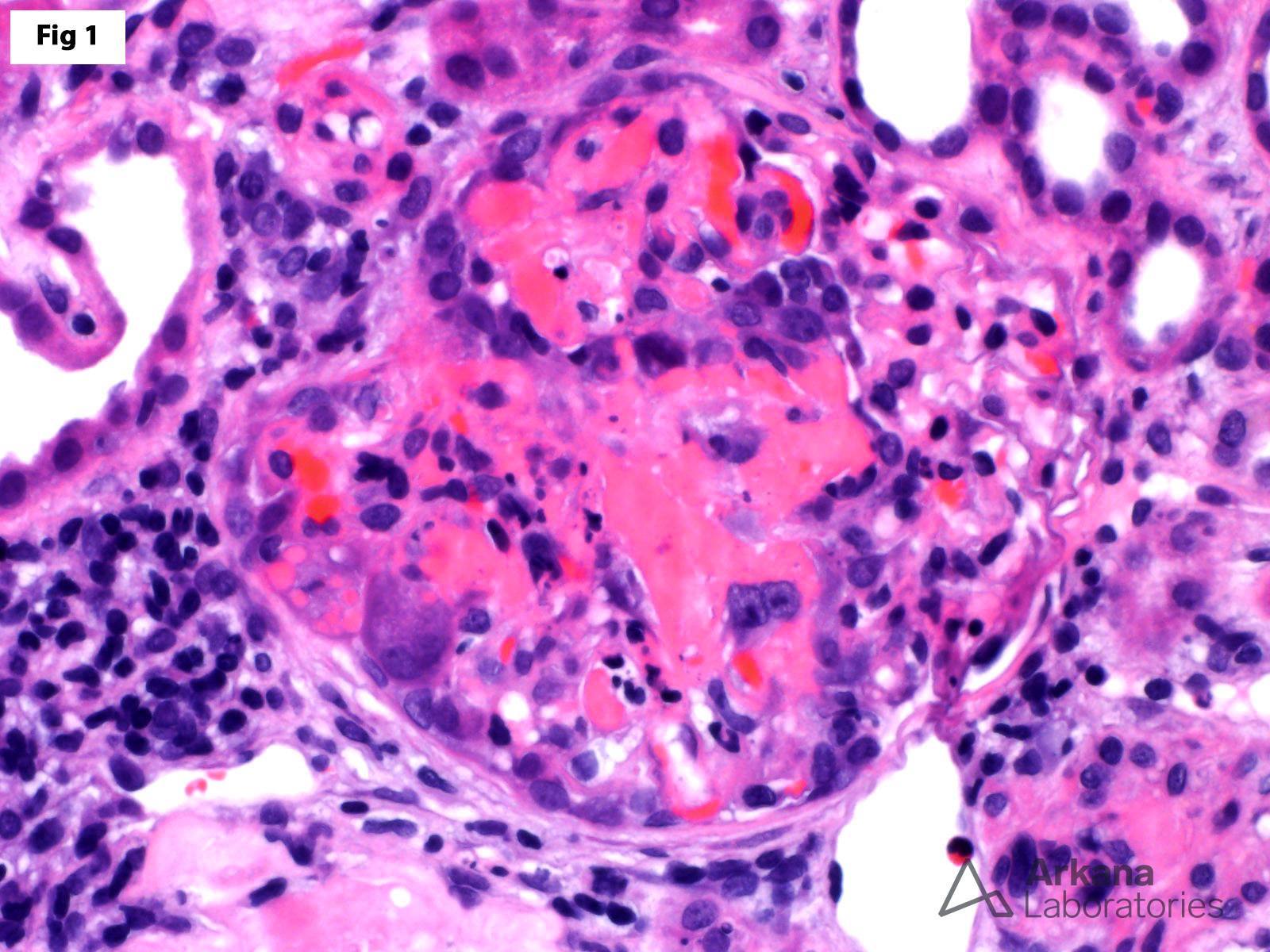
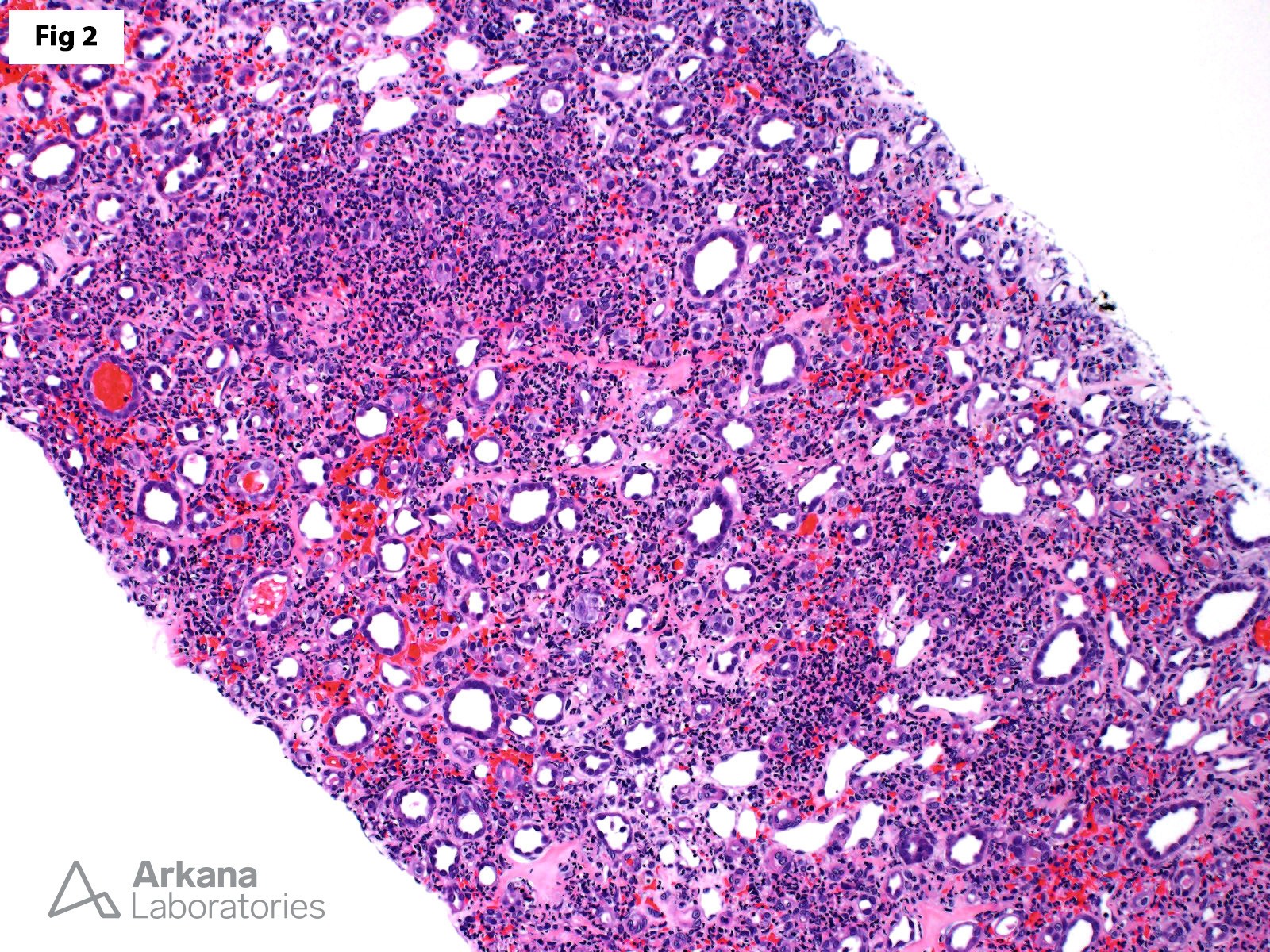
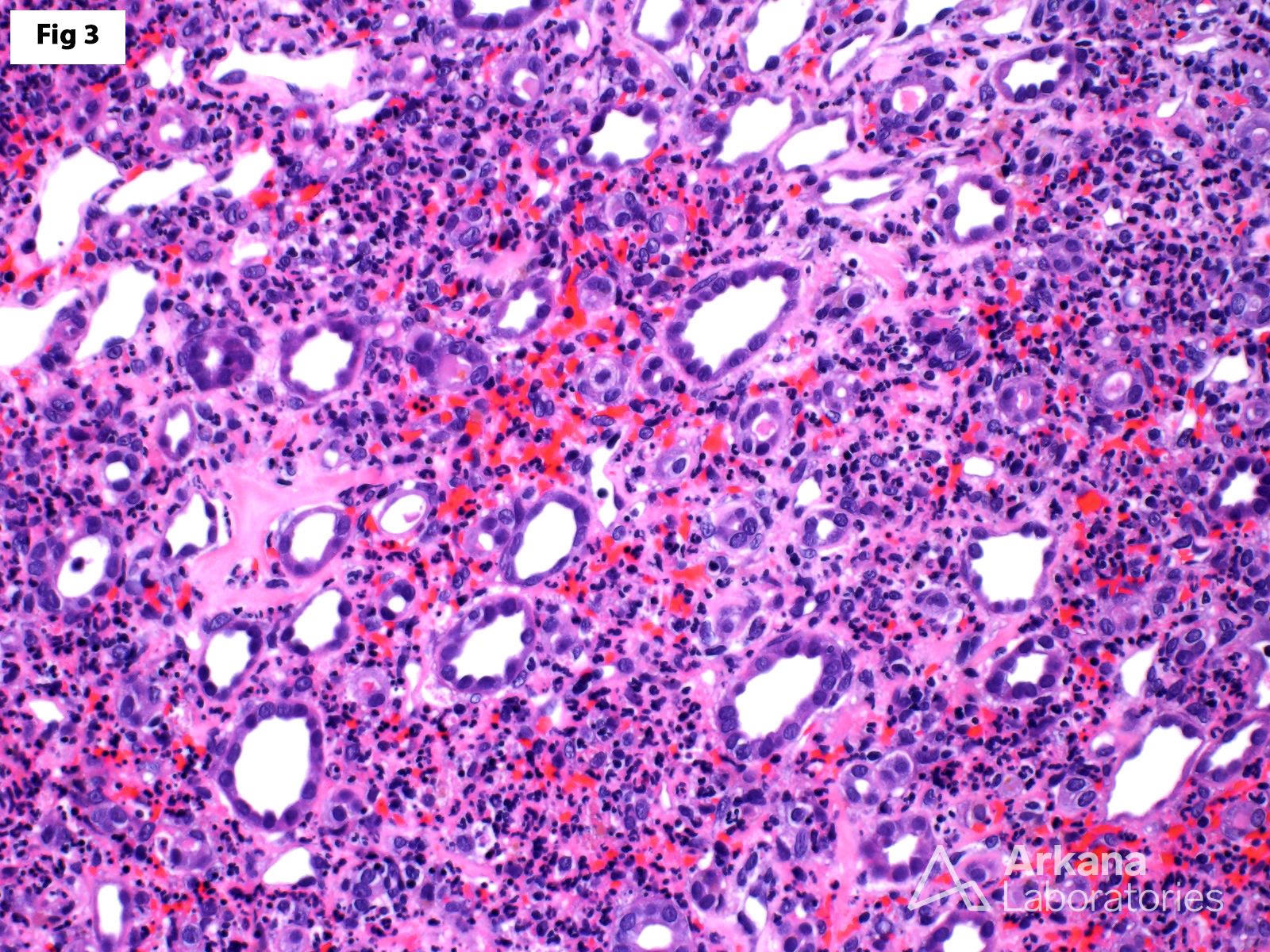
This 56-year-old female presented with acute kidney injury, hematuria, and mild proteinuria. All serologic studies were negative except for antineutrophil cytoplasmic antibodies (ANCA), which showed a perinuclear pattern of staining. A renal biopsy shows focal necrotizing and crescentic glomerulonephritis (Fig 1) with the absence of significant staining by immunofluorescence, consistent with ANCA-associated glomerulonephritis. Interestingly, the biopsy also shows significant neutrophil-rich medullary angiitis (Fig 2 and Fig 3). Medullary angiitis is characterized by the presence of interstitial hemorrhage, polymorphonuclear leukocyte infiltration, and karyorrhectic debris within the renal medulla. The morphology of medullary angiitis may be quite variable, mainly related to the extent and severity of each of these individual findings. This case, in particular, shows predominantly neutrophilic inflammation, disproportionate to the degree of interstitial hemorrhage and karyorrhectic debris. While the differential diagnosis would include an acute interstitial nephritis secondary to an ascending urinary tract infection (acute pyelonephritis), the absence of significant neutrophilic tubulitis, neutrophilic casts and the history of negative urine cultures makes this possibility much less likely. In addition to ANCA-associated glomerulonephritis, medullary angiitis may also be seen in the setting of IgA nephropathy, and in patients with infections receiving antibiotics.
Reference:
Hendricks AR, Harris AA, Walker PD, Larsen CP. Renal medullary angiitis: a case series from a single institution. Hum Pathol. 2013 Apr;44(4):521-5.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.