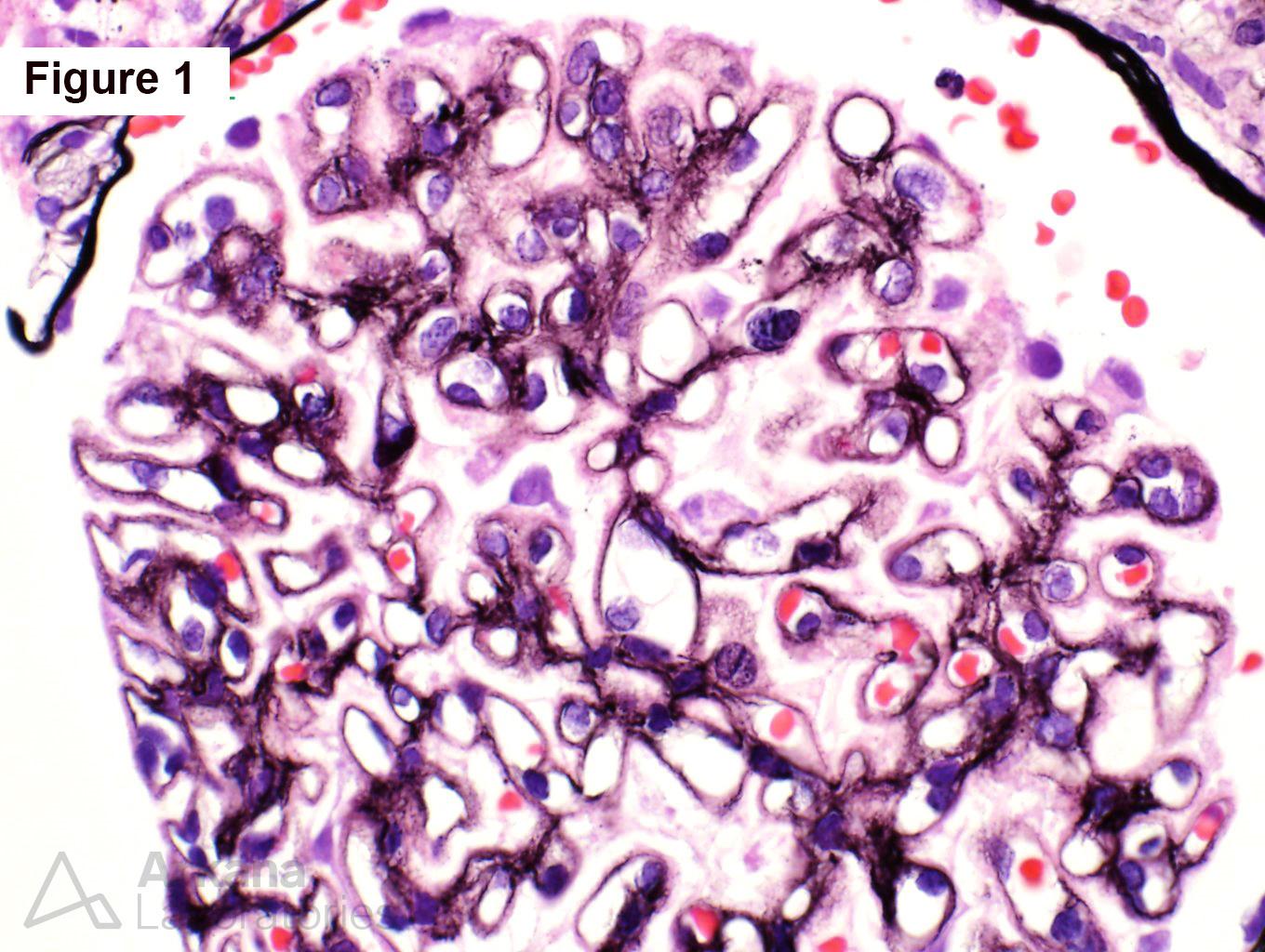
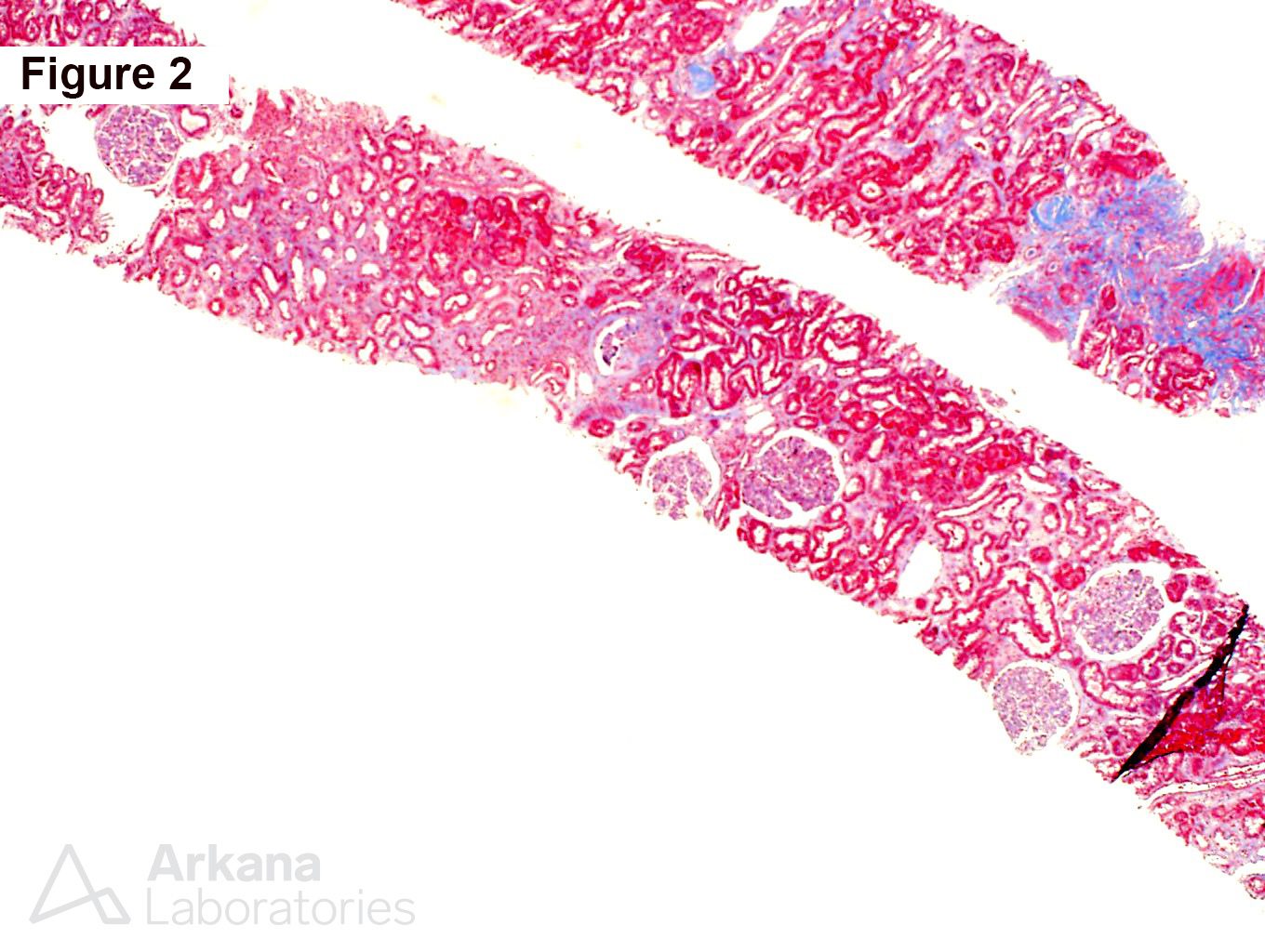
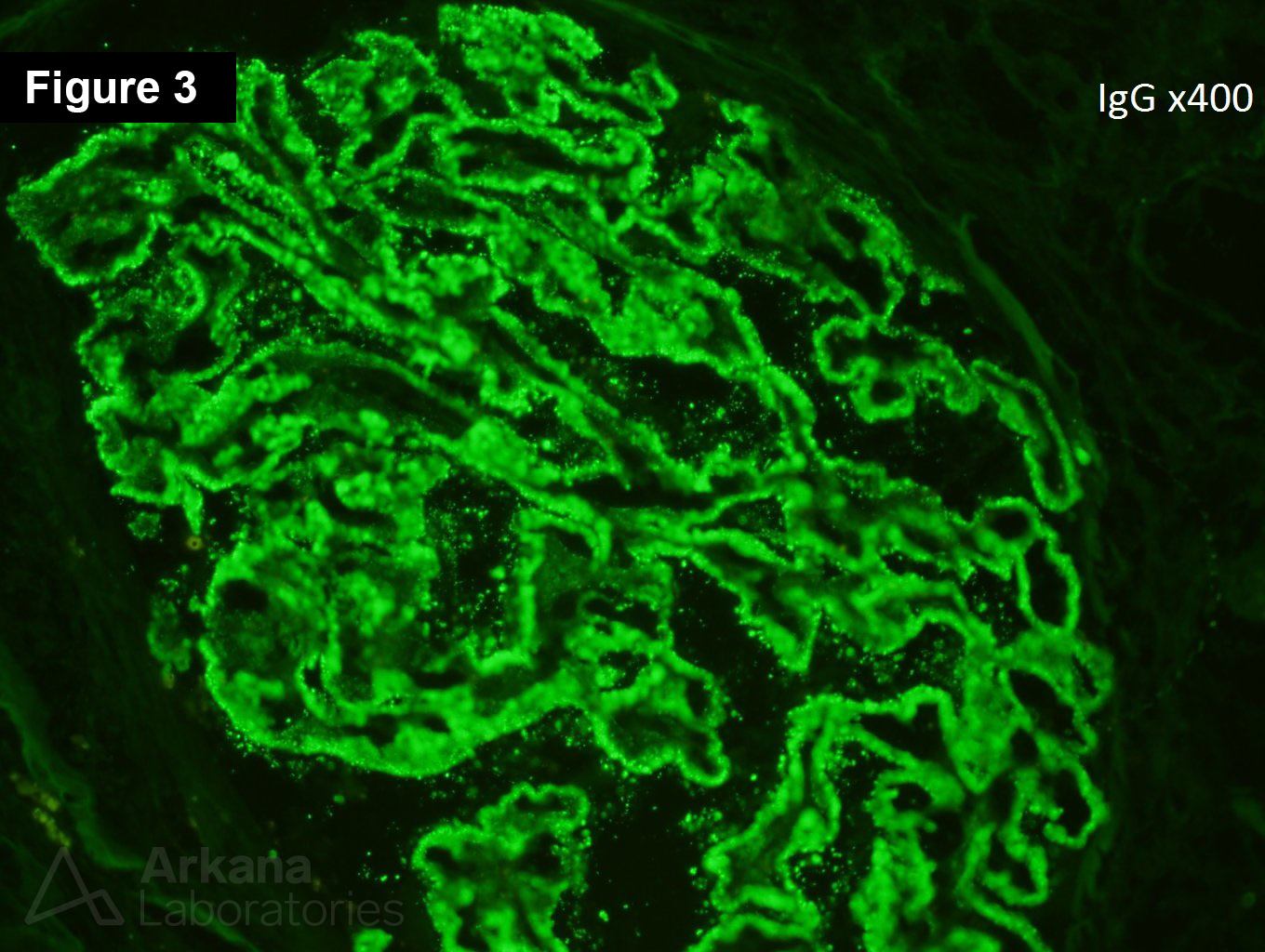
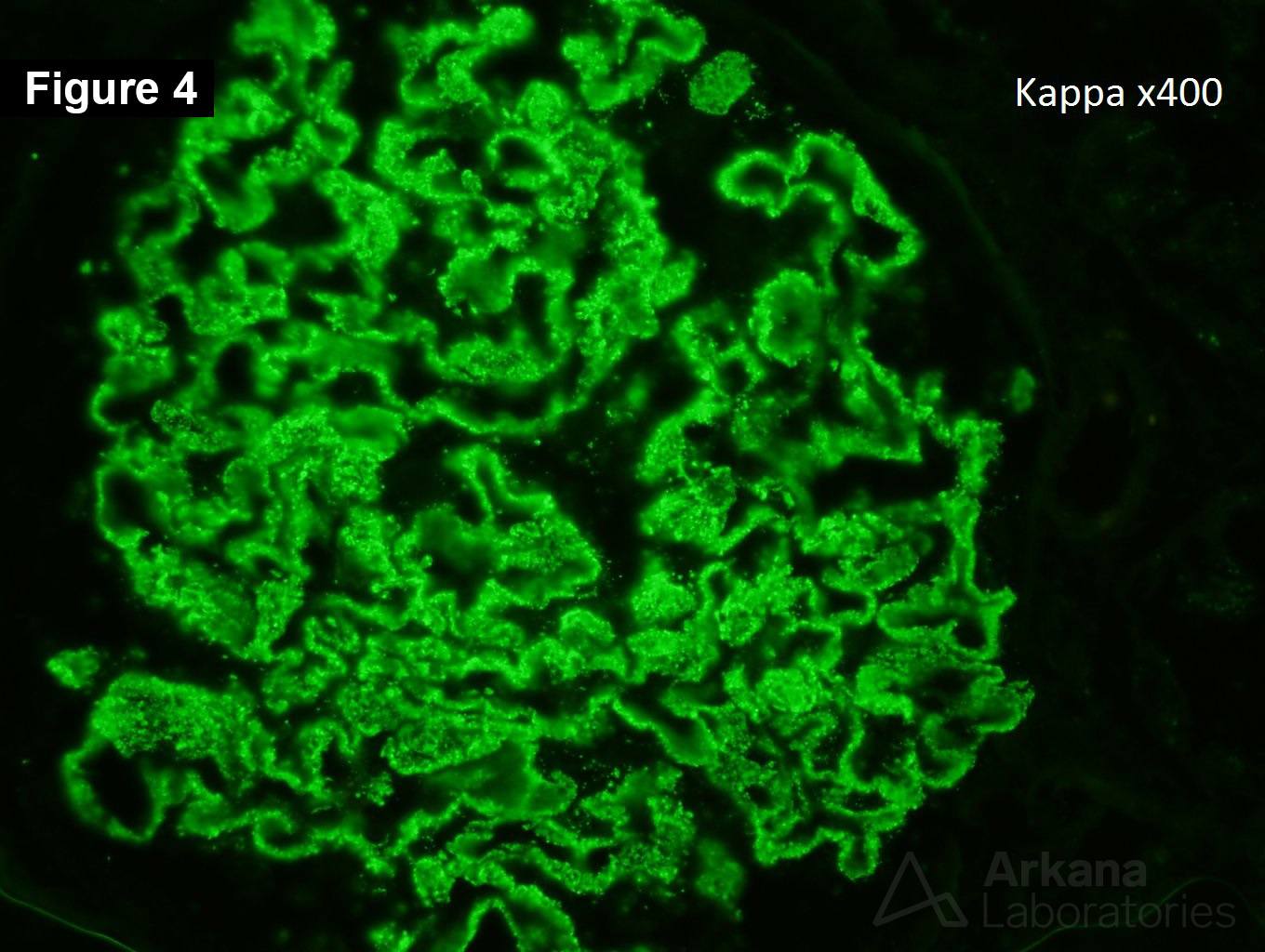
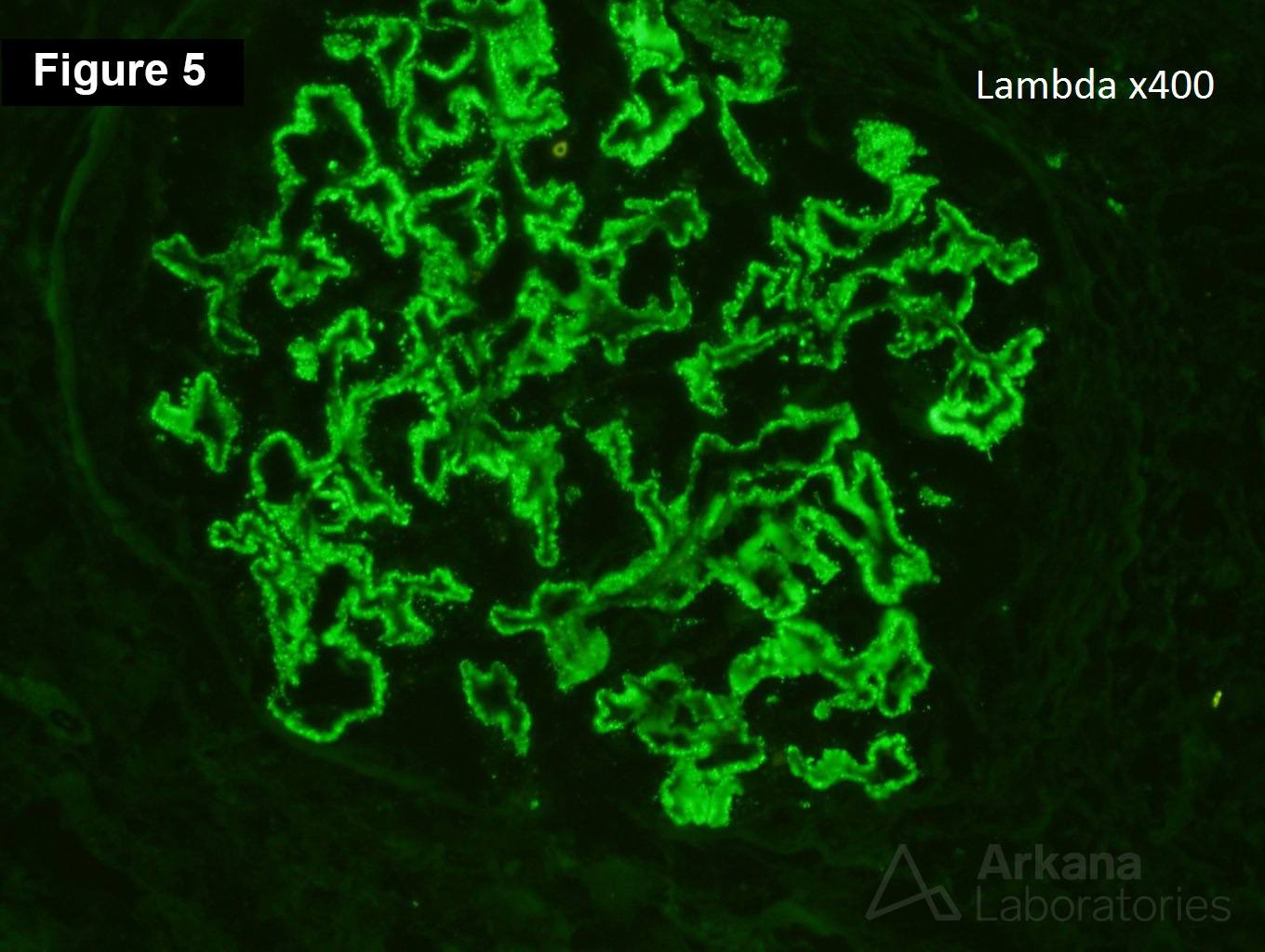
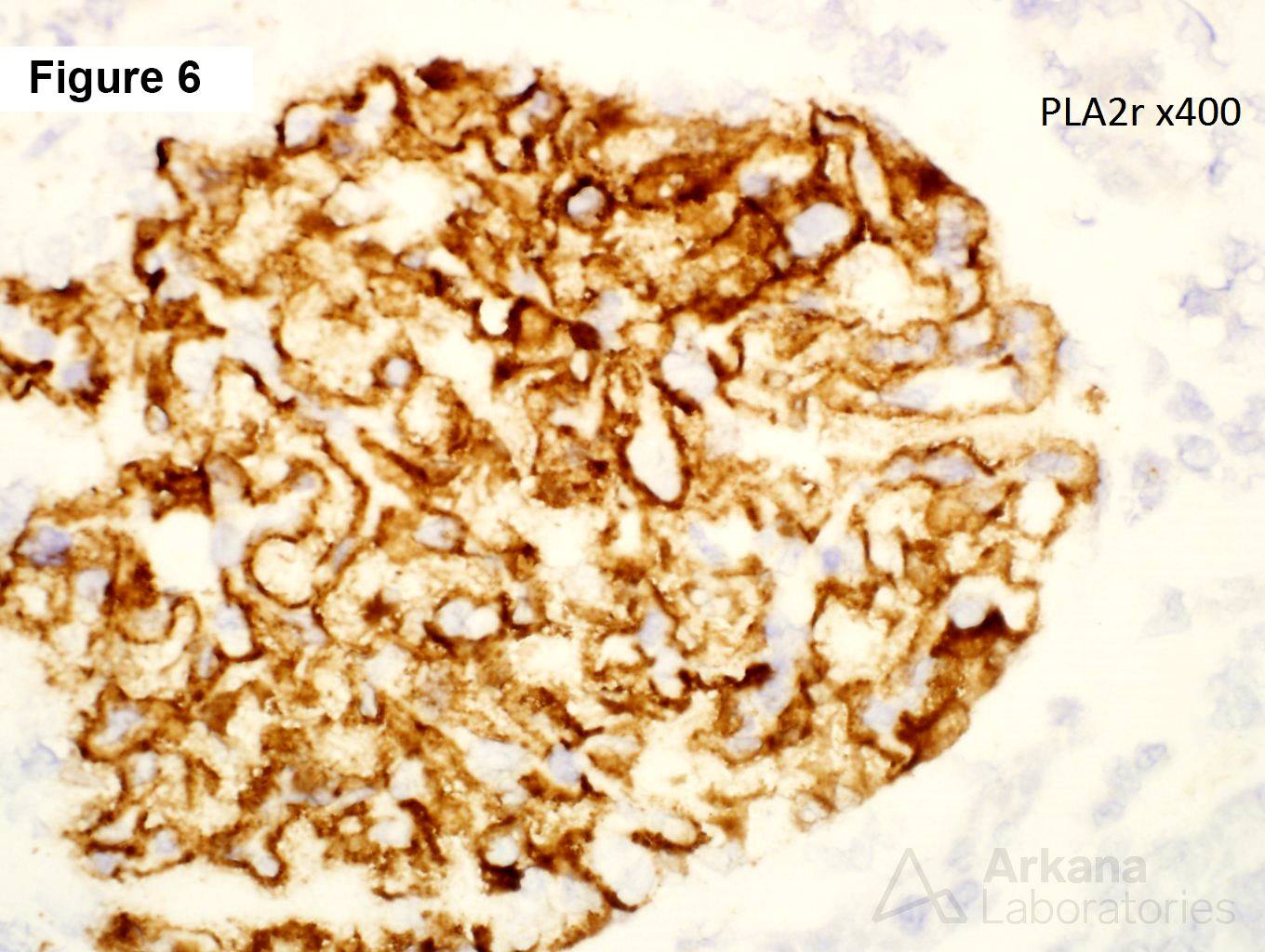
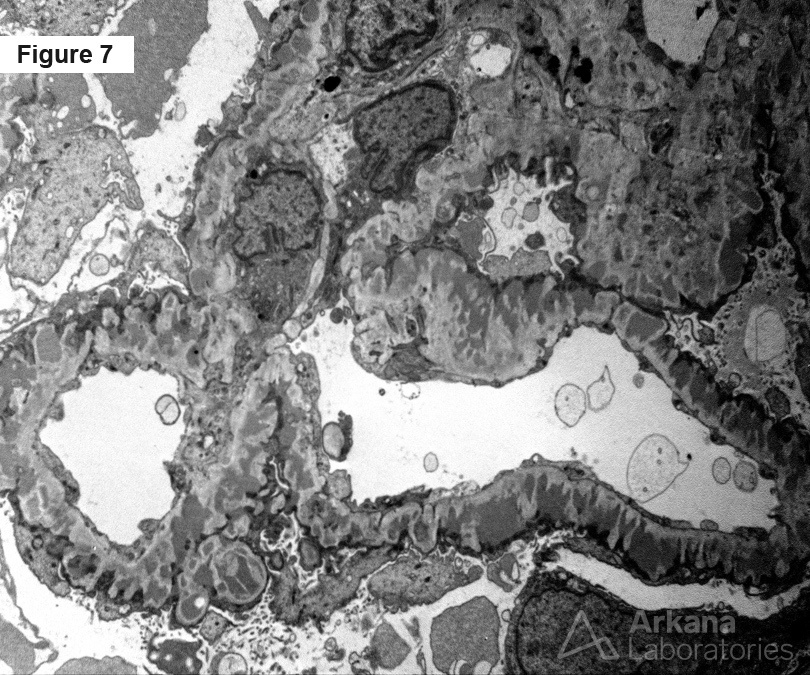
The biopsy shows a recurrent membranous nephropathy within a transplant. Figure 1 shows “spikes” and “holes.” Figure 2 shows mild interstitial fibrosis. Figures 3, 4, 5, and 6 shows IgG, kappa, lambda, and PLA2r, respectively. Figure 7 shows subepithelial and intramembranous deposits.
Membranous nephropathy can arise in the graft from recurrence of the original disease, a de novo disease, and rarely as a donor-derived disease. Recurrence of the original disease can be seen as early as one week post transplant. Most cases of recurrent membranous nephropathy occur within the first few months following transplantation, whereas de novo membranous nephropathy usually appears after the first year (or many years). Recurrent membranous nephropathy is usually PLA2r positive, while de novo disease is usually PLA2r negative. It is recommended to follow anti-PLA2r levels in patients with primary membranous nephropathy when they receive a transplant. Especially, as recurrent membranous nephropathy appears to reach end-stage renal disease more often than primary membranous, even in cases of non-aggressive disease at diagnosis. Unlike the native kidney, there is a lower chance of spontaneous remission in the transplant kidney and a greater requirement for adjuvant immunosuppressive therapy to induce remission.
https://www.ncbi.nlm.nih.gov/pubmed/30985736
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.