Clinical History
The 21-year-old patient presented with skin rash and proximal upper and lower extremity weakness of several weeks duration. Laboratory studies showed elevated CPK (12000 to 14000 range). Myositis specific autoantibody panel test results were pending. The patient was not treated with steroid prior to muscle biopsy.
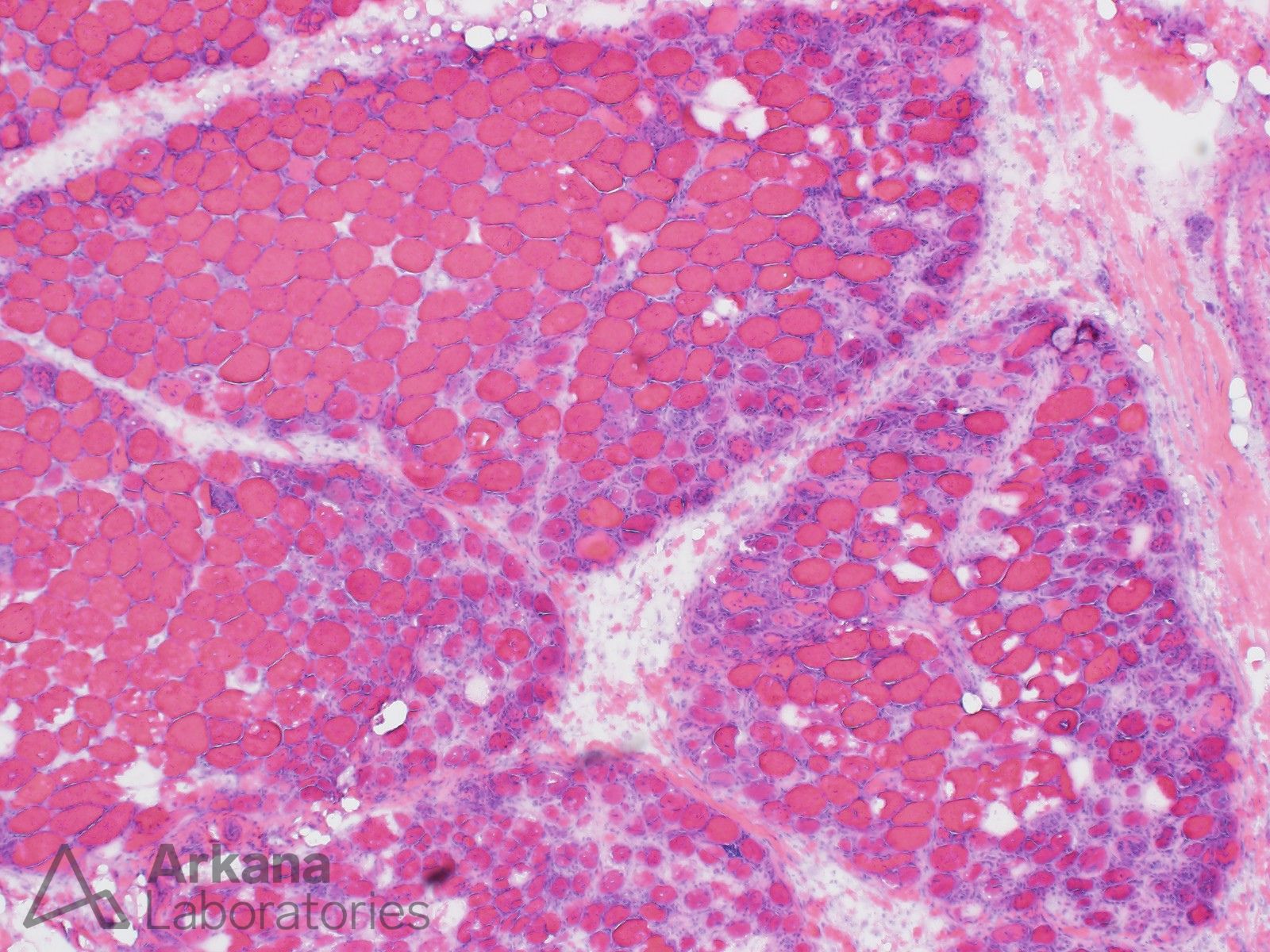
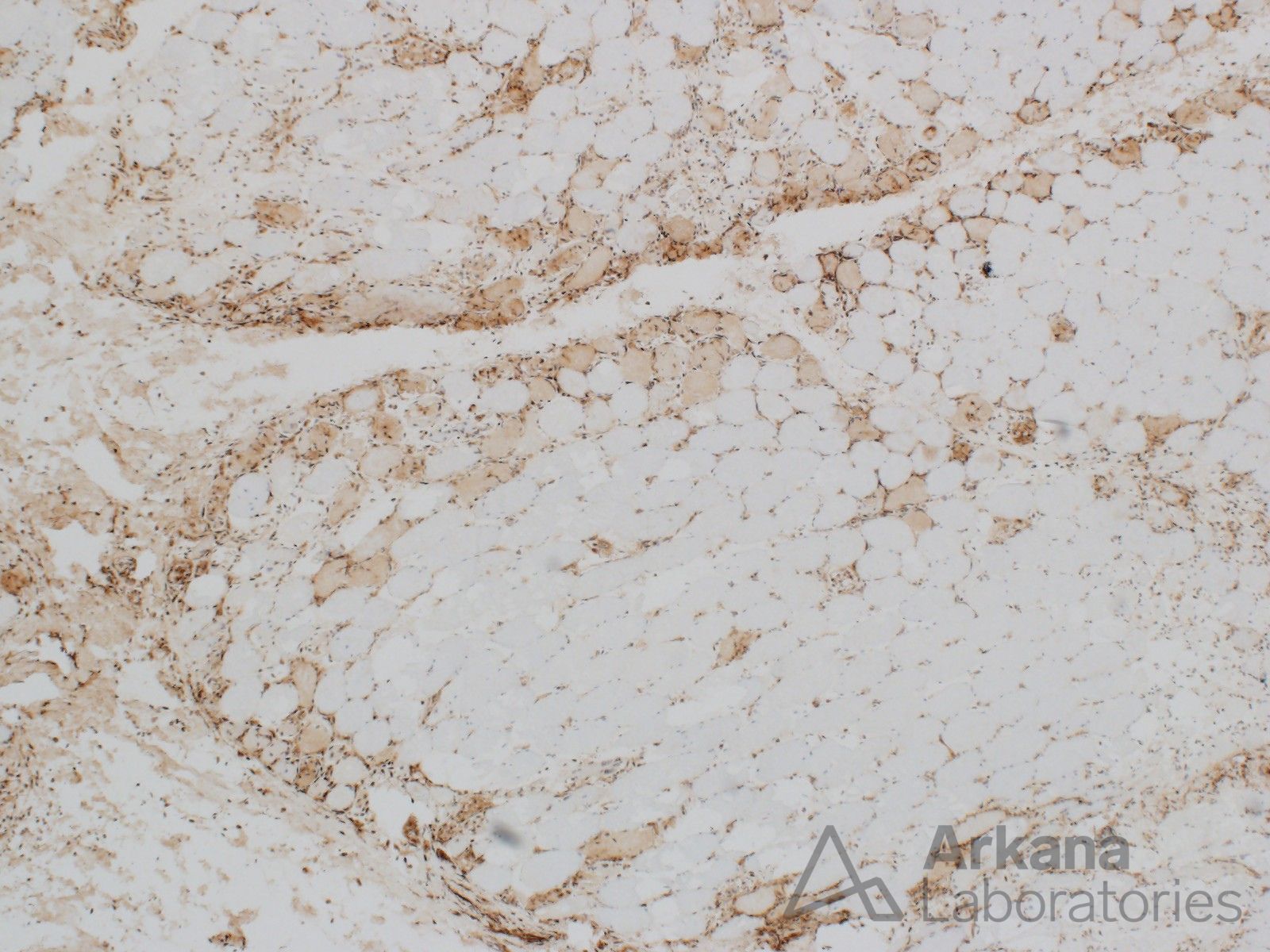
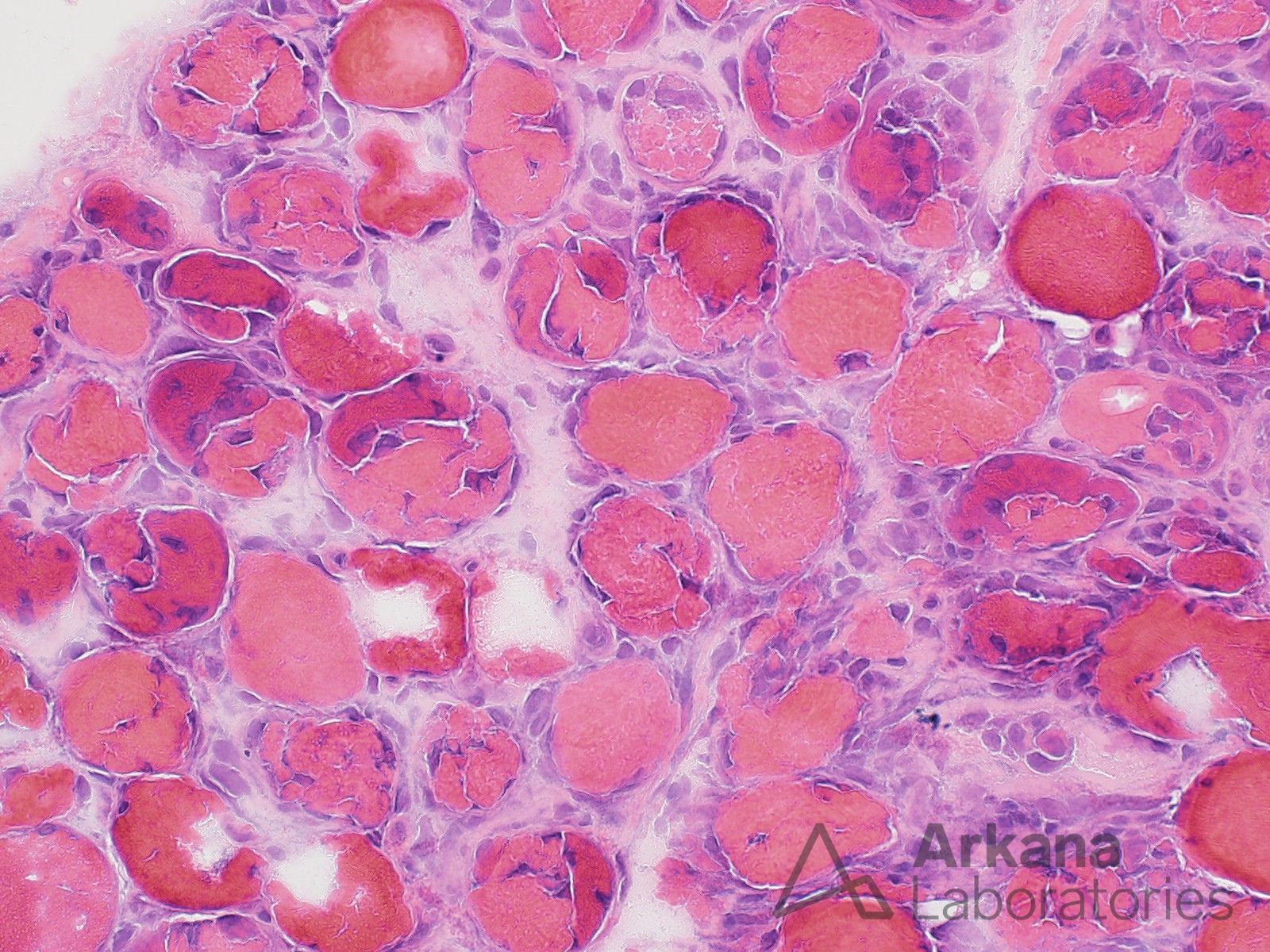
What is your diagnosis based on the provided H&E and MxA stains sections? How would you characterize the damaged myofibers in the higher power H&E image?
Answer:
- The pathologic changes are most consistent with the presence of dermatomyositis (inflammatory myopathy with perifascicular pattern of myofiber injury and perifascicular pattern of myofiber staining for MxA (myxovirus resistance protein A). However, correlation with myositis specific autoantibody panel test results is needed as a perifascicular pattern of myofiber injury may also be seen in anti-synthetase syndrome.
- The damaged myofibers show a morphologic spectrum ranging from basophilic regenerating, necrotic, and partially necrotic partially regenerating. This likely represents cross sectional sampling of segmental/patchy myofiber necrosis. Some neuromuscular specialists separate “perifascicular atrophy” from “perifascicular necrosis.”
Reference(s)/Additional Reading:
- Xing C, Trivedi J, Bitencourt N, Burns DK, Reisch JS, Cai C. Myxovirus resistance protein A (MxA) expression in myositides: Sarcoplasmic expression is common in both dermatomyositis and lupus myositis. Muscle Nerve. 2024 May;69(5):548-555. doi: 10.1002/mus.28066. Epub 2024 Feb 19. PMID: 38372203.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.