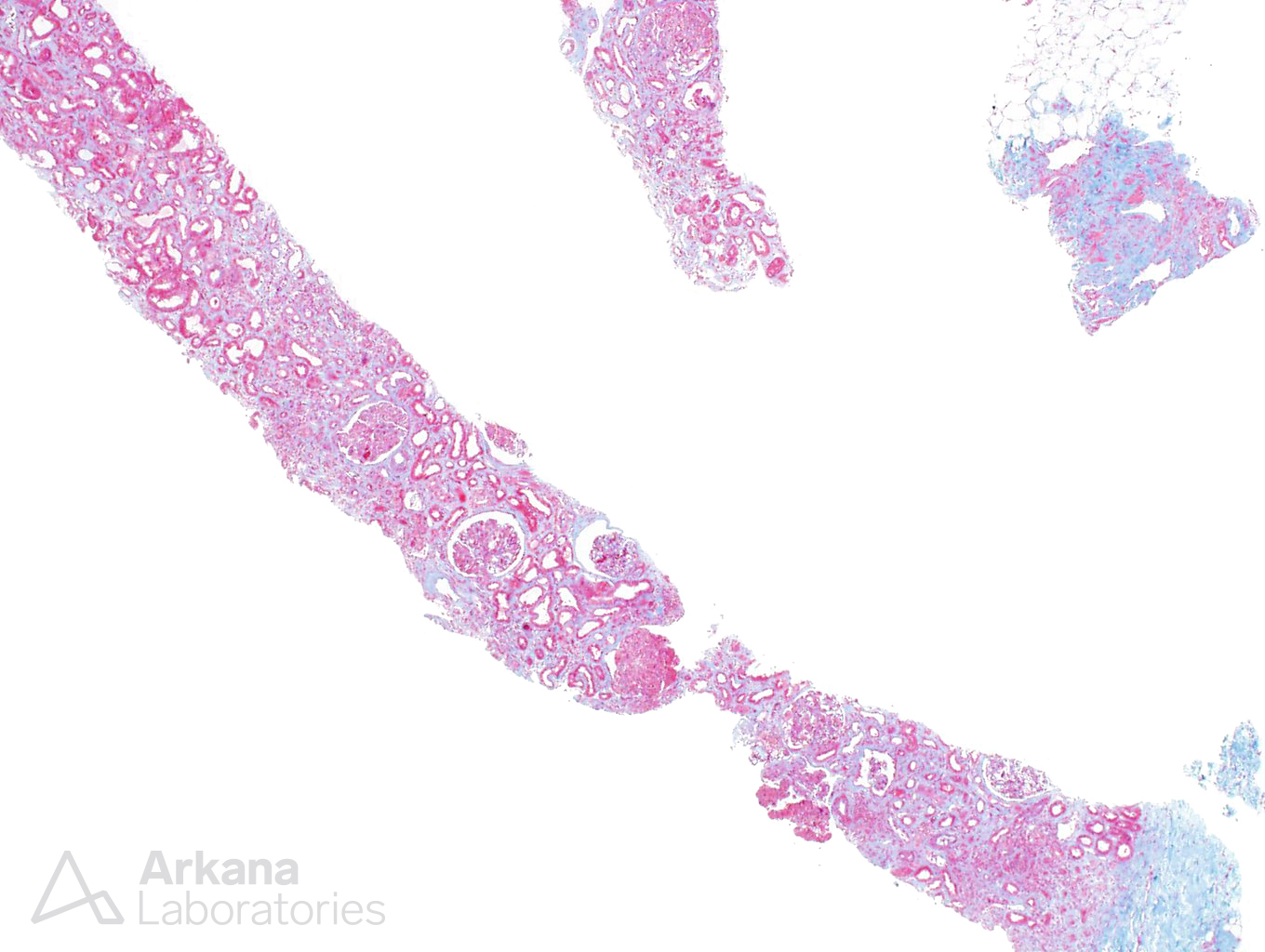
A 65-year-old male presents with mild proteinuria and a sudden increase in creatinine. He was recently diagnosed with widely metastatic gastric carcinoma and has received 4 rounds of chemotherapy. During treatment with chemotherapy, his creatinine increased to 3.5 and has remained at that level despite fluid resuscitation. A kidney biopsy is performed.
What is the best diagnosis?
A. Membranoproliferative Glomerulonephritis
B. Metastatic Gastric Carcinoma
C. Intravascular Diffuse Large B-Cell Lymphoma
D. Thrombotic Microangiopathy
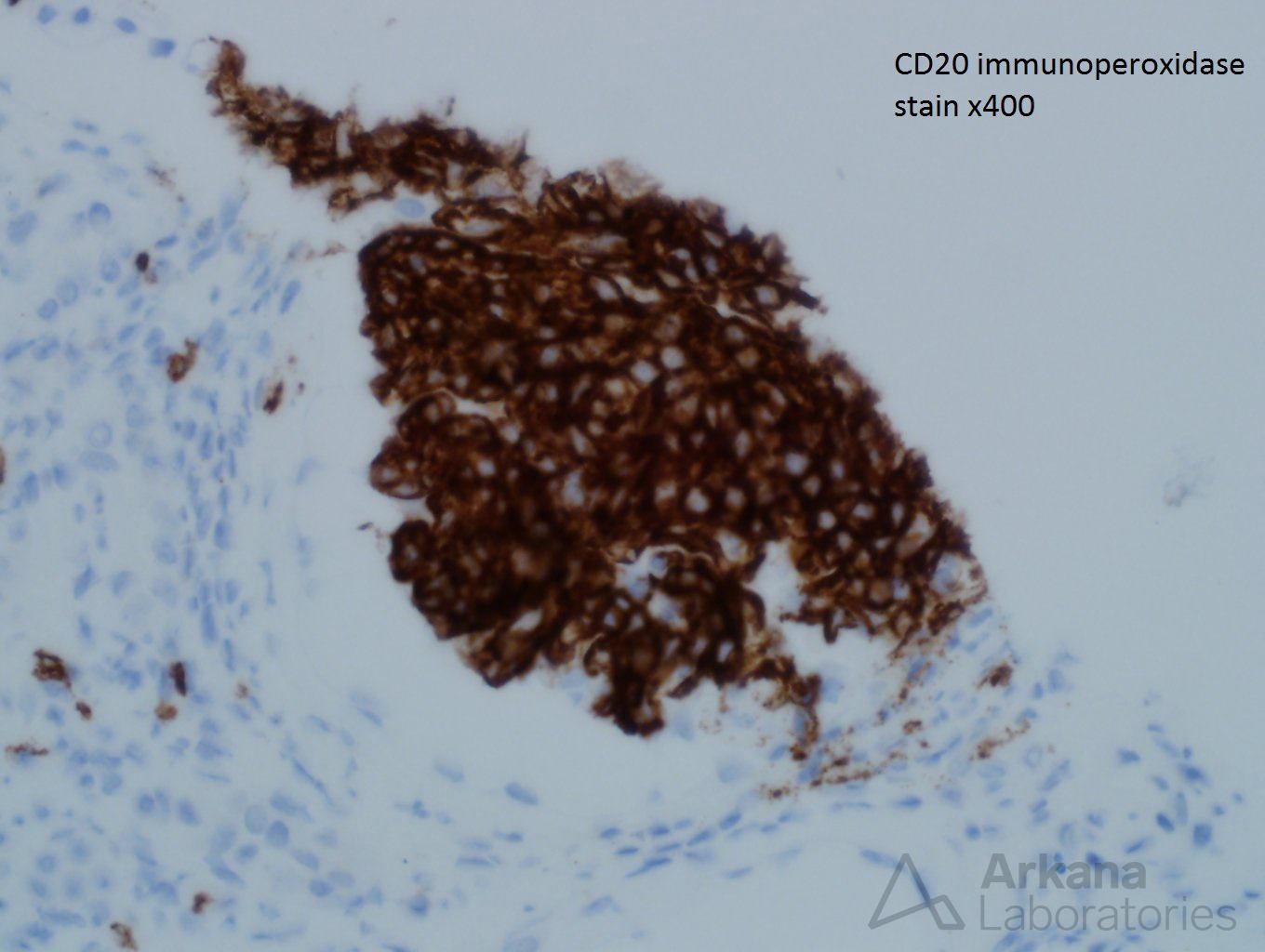
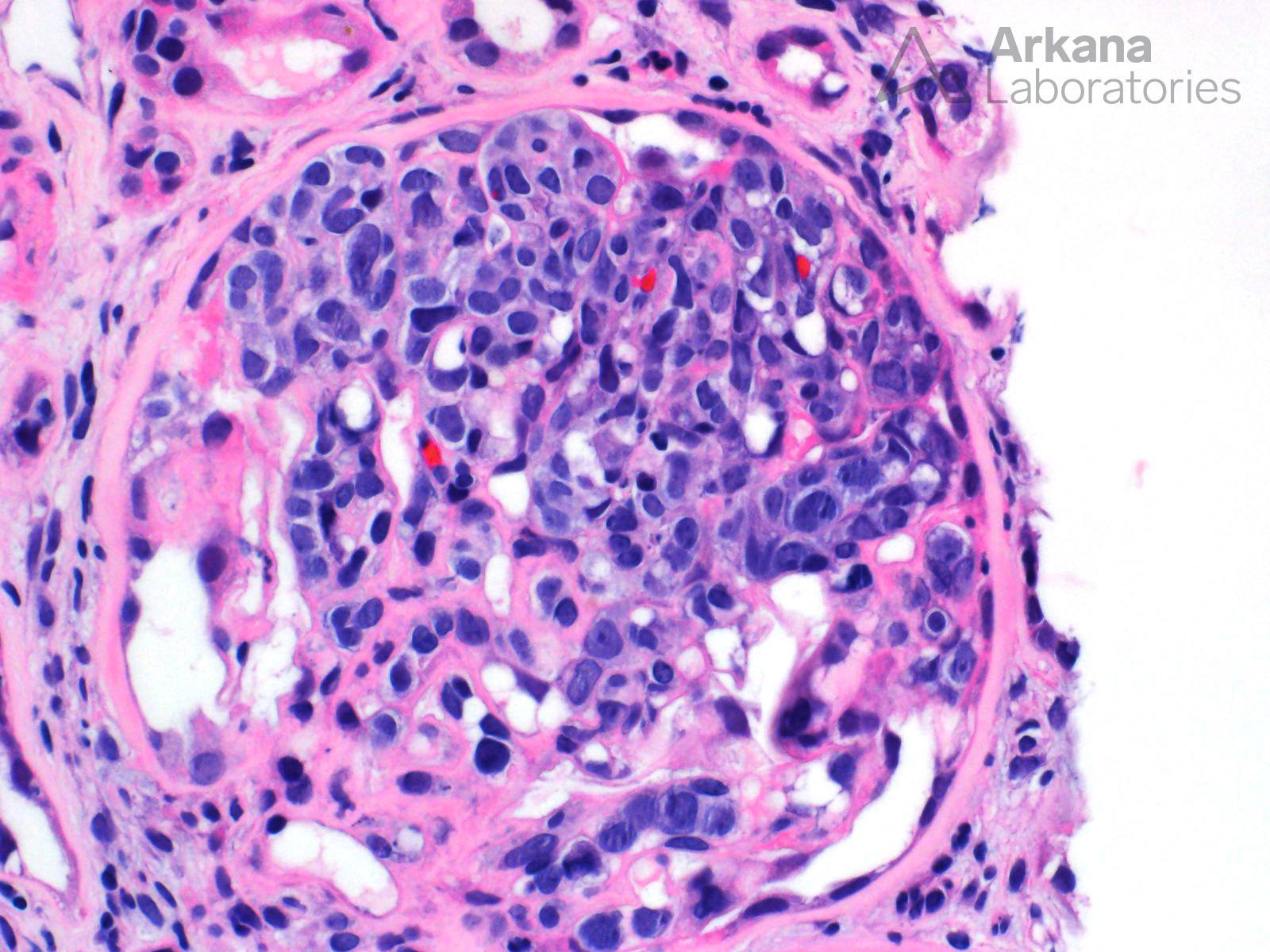
The best answer is C – Intravascular Diffuse Large B-Cell Lymphoma
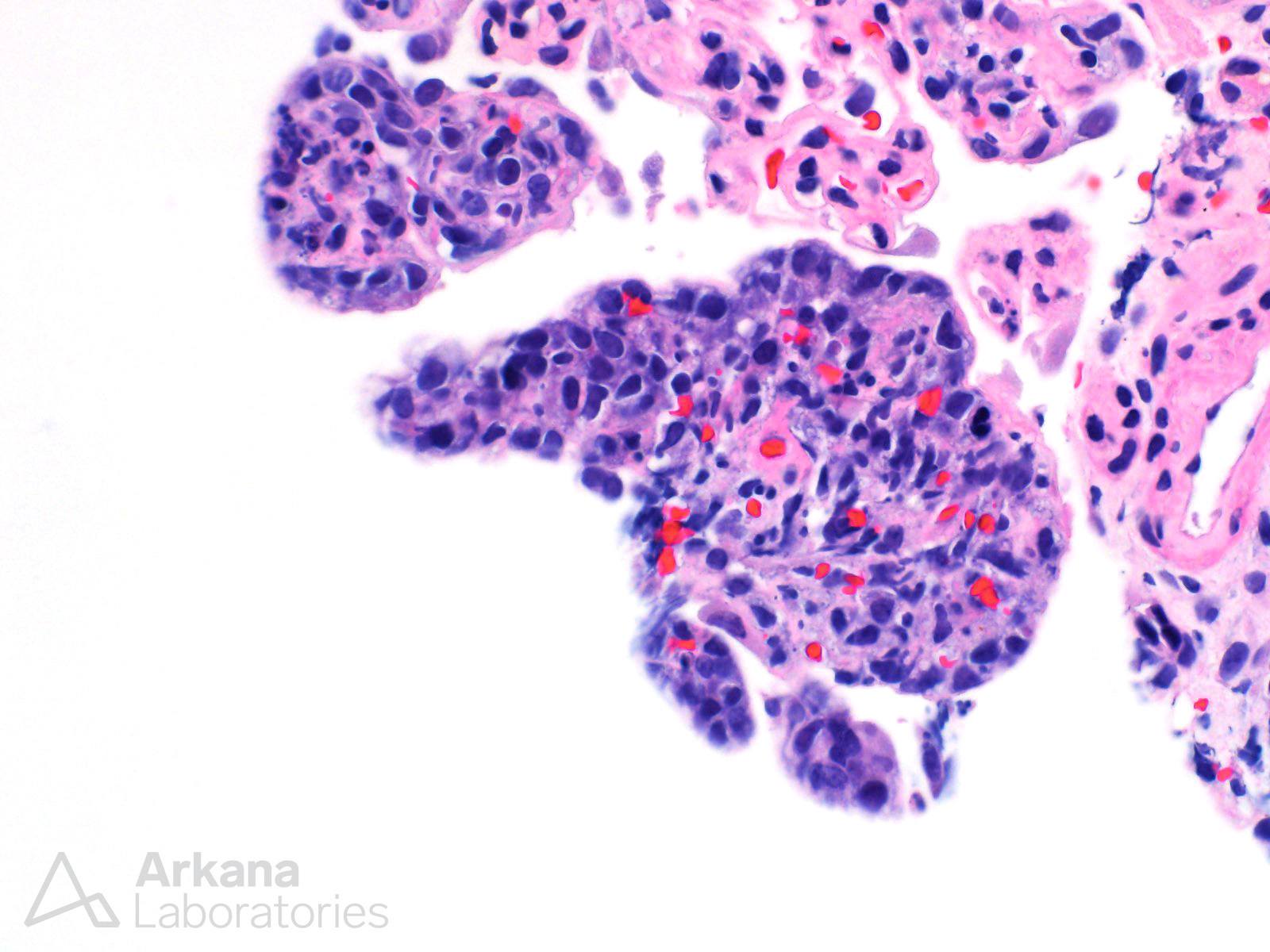
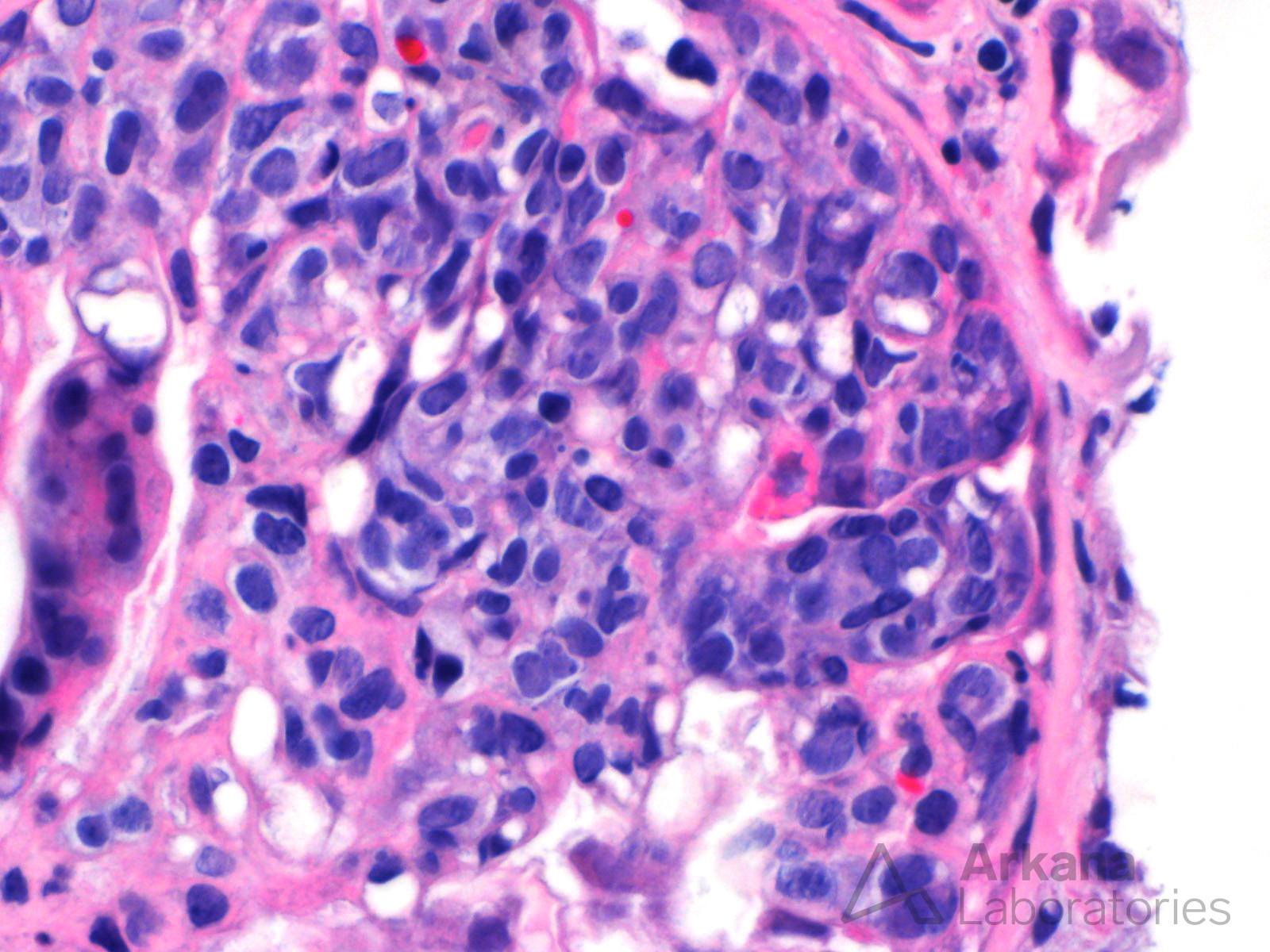
This is a very difficult case due to the proliferative nature of the glomeruli. At first glance, this looks like a membranoproliferative glomerulonephritis due to the presence of both mesangial and endocapillary hypercellularity. On closer inspection of the intracapillary cells, it becomes apparent that they are atypical and dysplastic. The clustering of the cells and the presence of signet-ring cells makes the argument toward metastatic gastric carcinoma (especially with the history). However, the positive CD20 stain and the negative pan-cytokeratin (not shown) confirms that this is a intravascular diffuse large B-cell lymphoma. Even though it is well known that chemotherapy can lead to thrombotic microangiopathy, the cellular nature of the glomeruli precludes this diagnosis.
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.