This biopsy is from a person in their 40’s, who presented with accelerated hypertension and blood pressure of 240/180 mm/Hg. Urinalysis showed 2+ protein and 2+ blood and his serum creatinine was 7.2 mg/dl. Further workup revealed a low platelet count at 90,000 and schistocytes on peripheral smear. He was admitted to the ICU where careful hypertension management was instituted. Serologies were negative for ANA, cANCA, pANCA, anti-GBM, and hepatitis B and C. Complements were normal. ADAMTS-13 was normal.
Diagnosis:
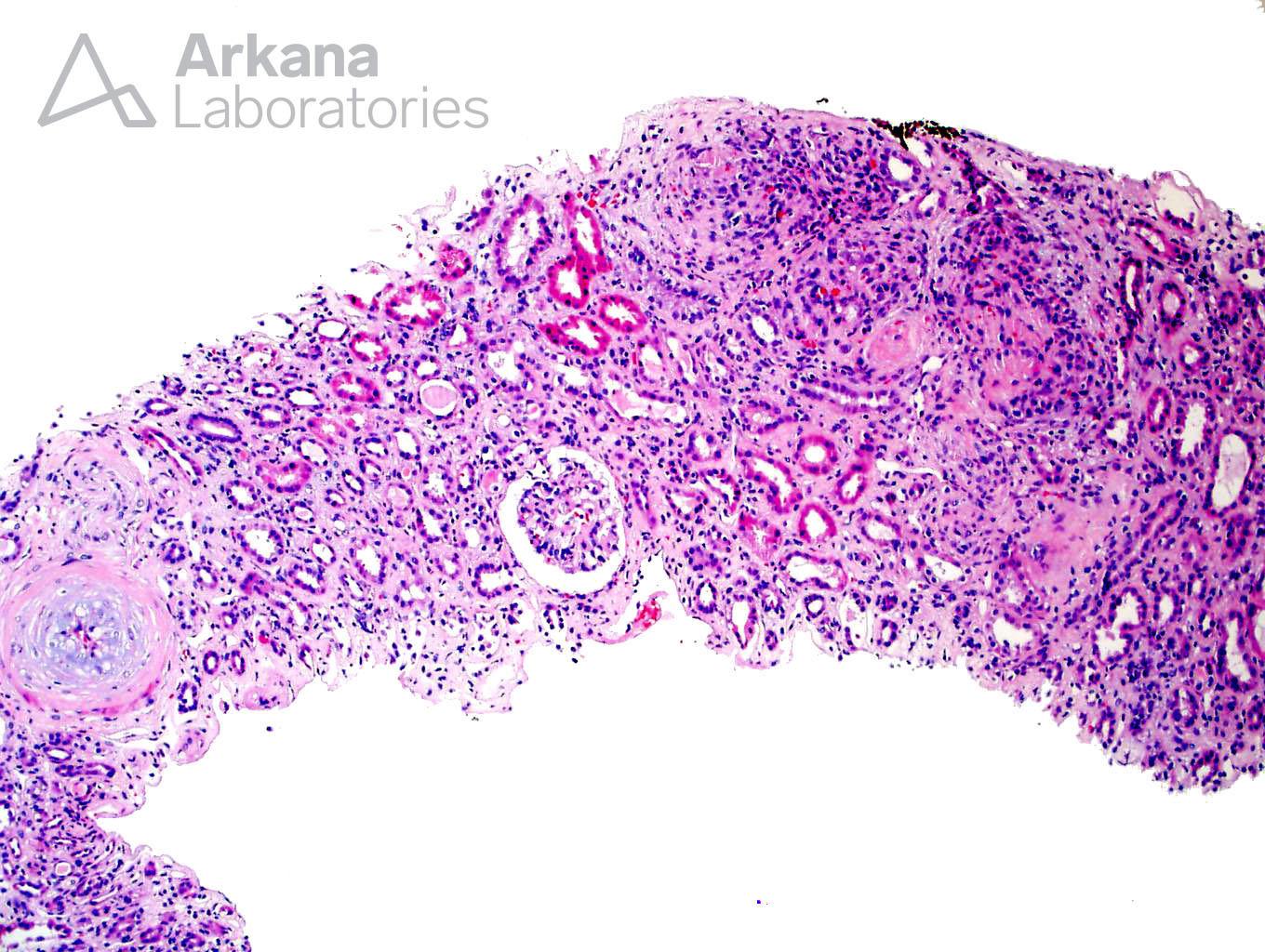
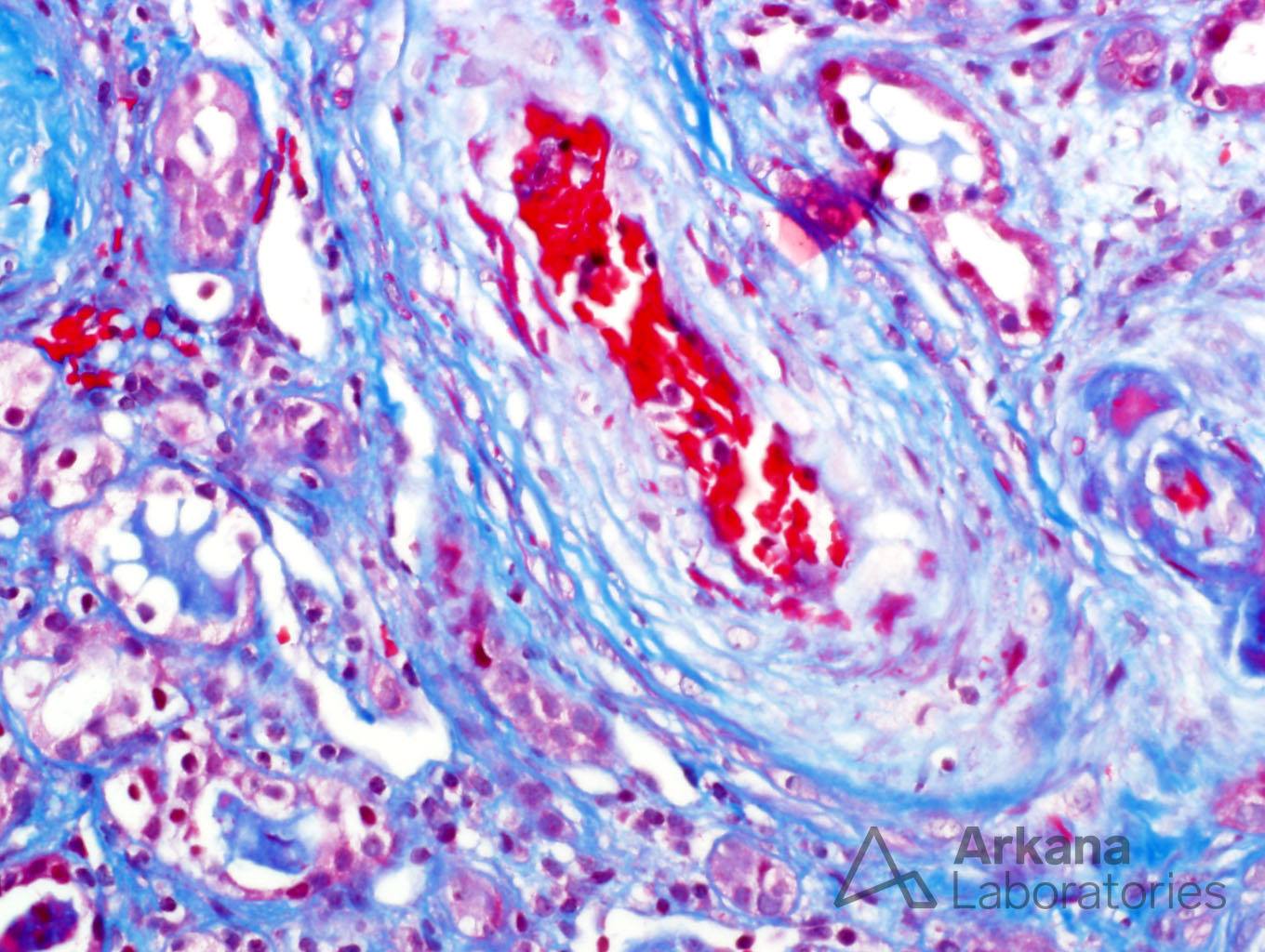
Thrombotic Microangiopathy
Global Glomerulosclerosis (20/72).
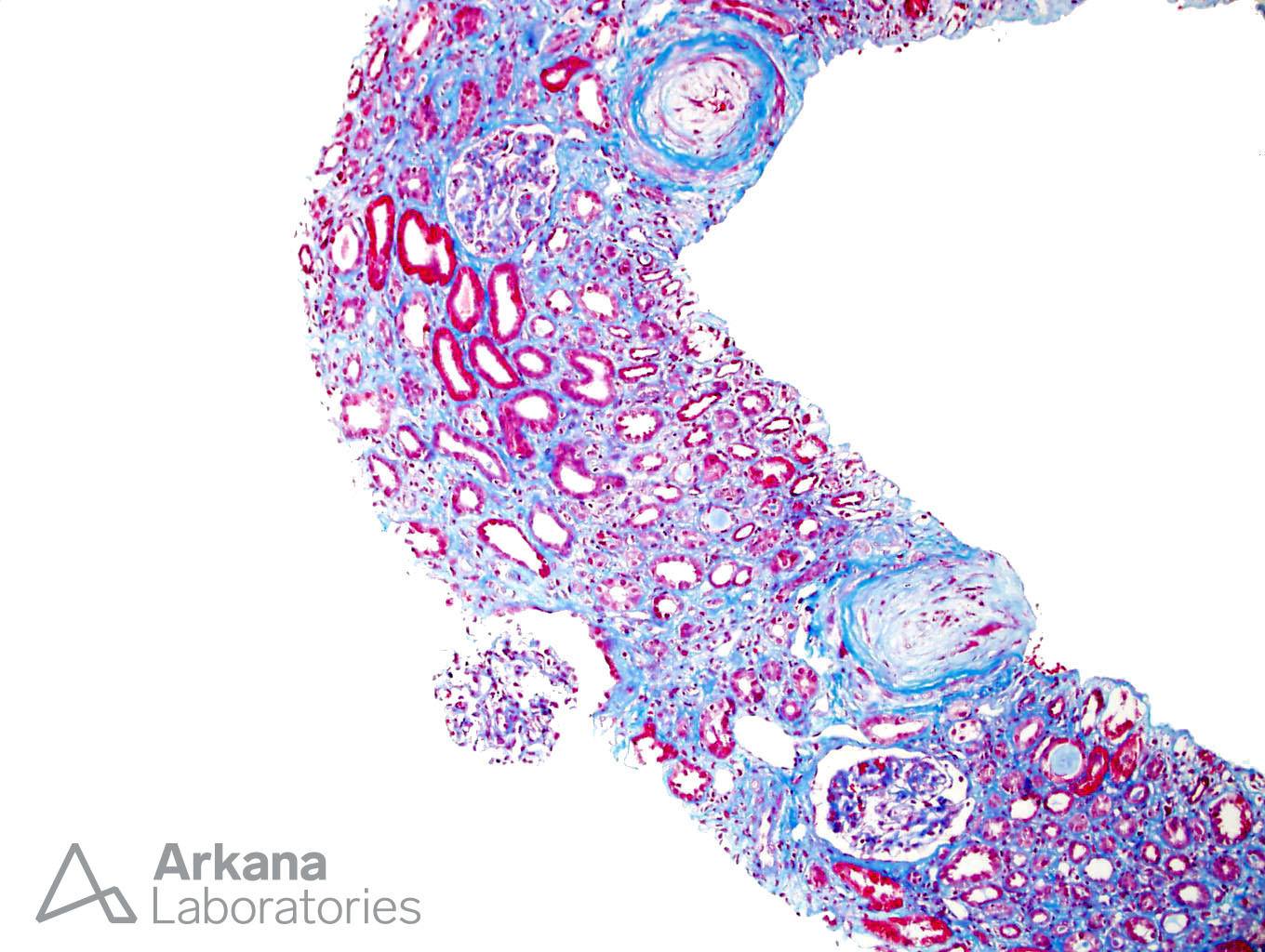
Interstitial Fibrosis, Severe.
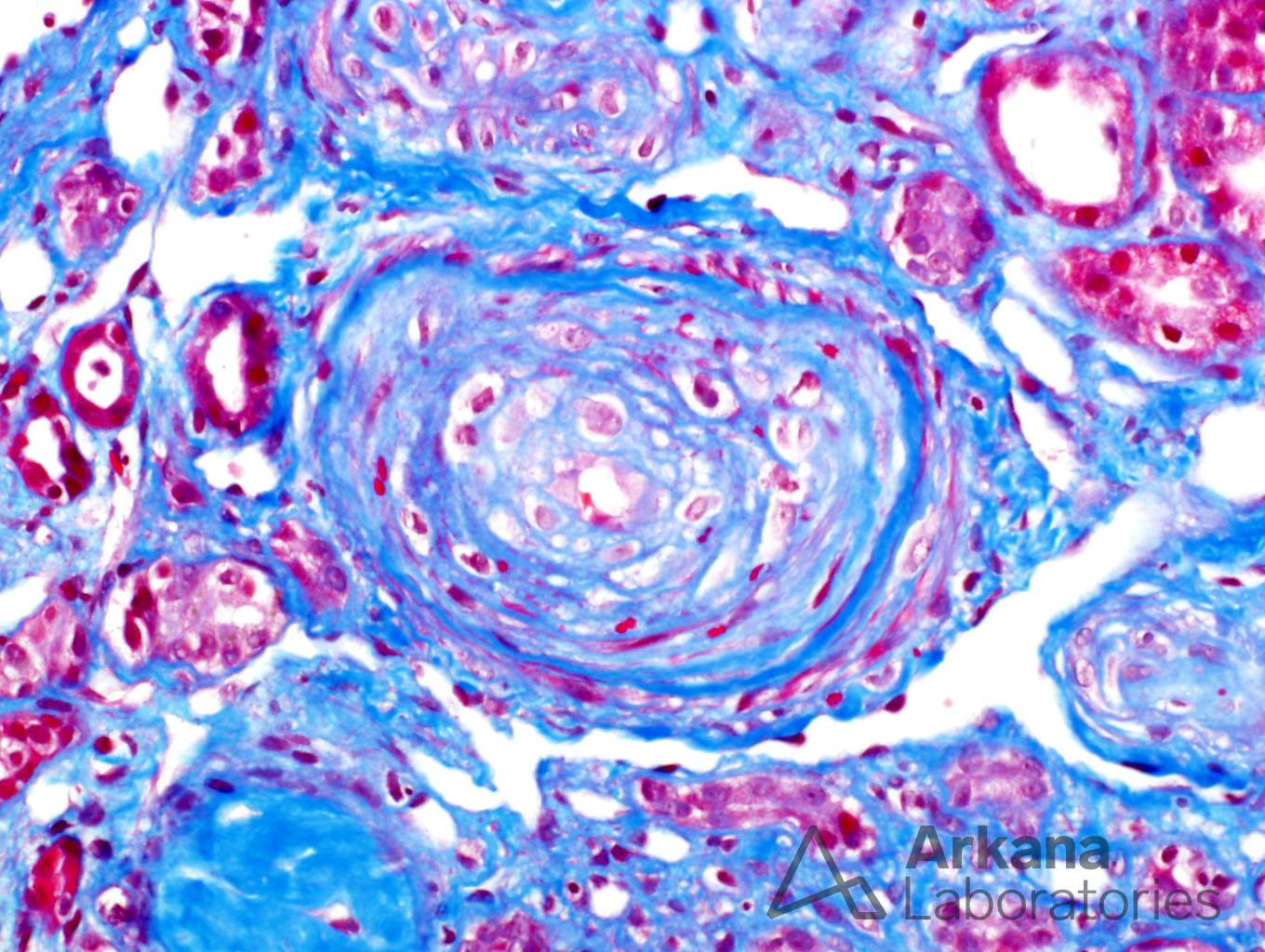
Arteriosclerosis and Arteriolar Hyalinosis, Severe.
Discussion:
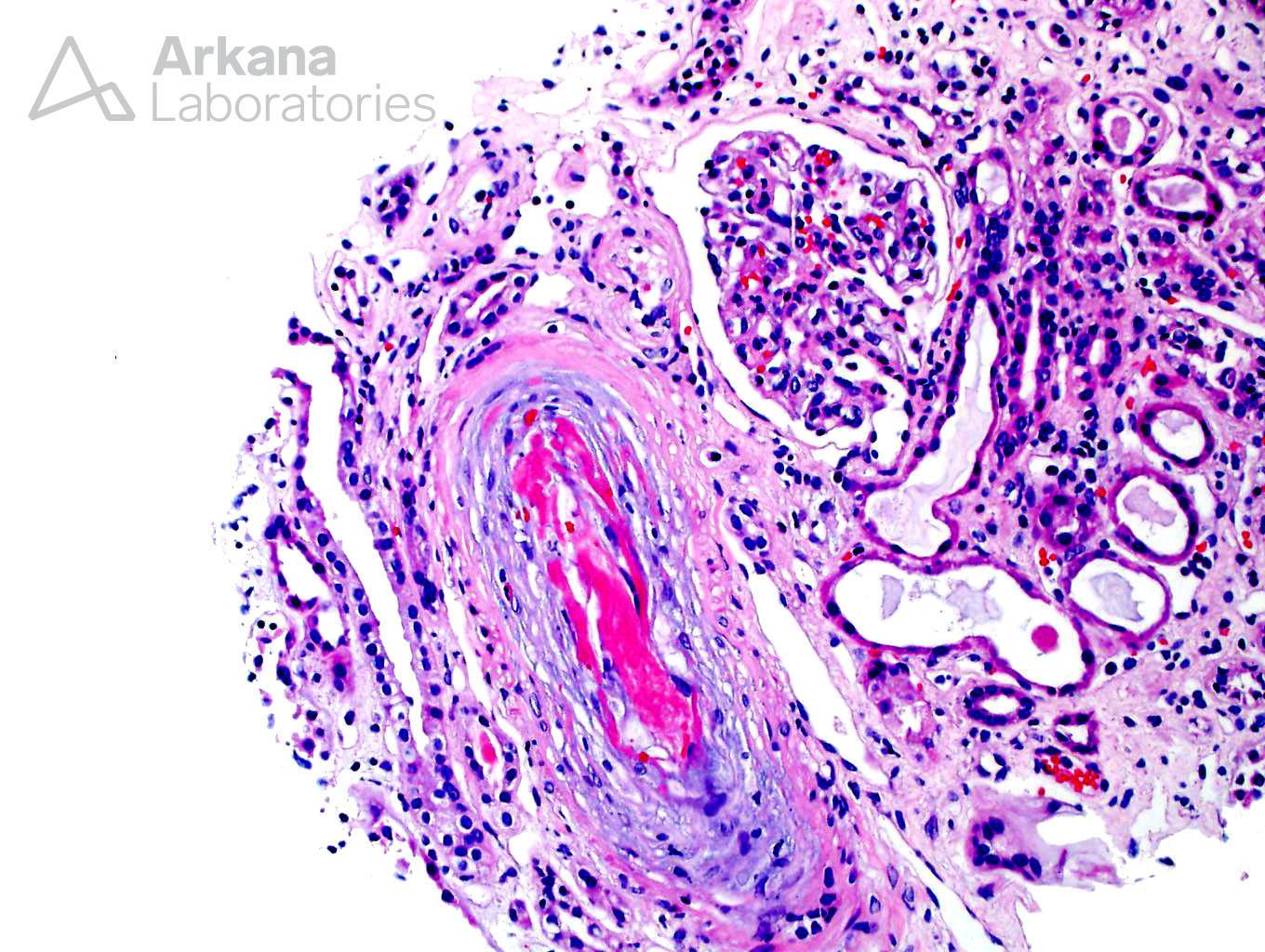
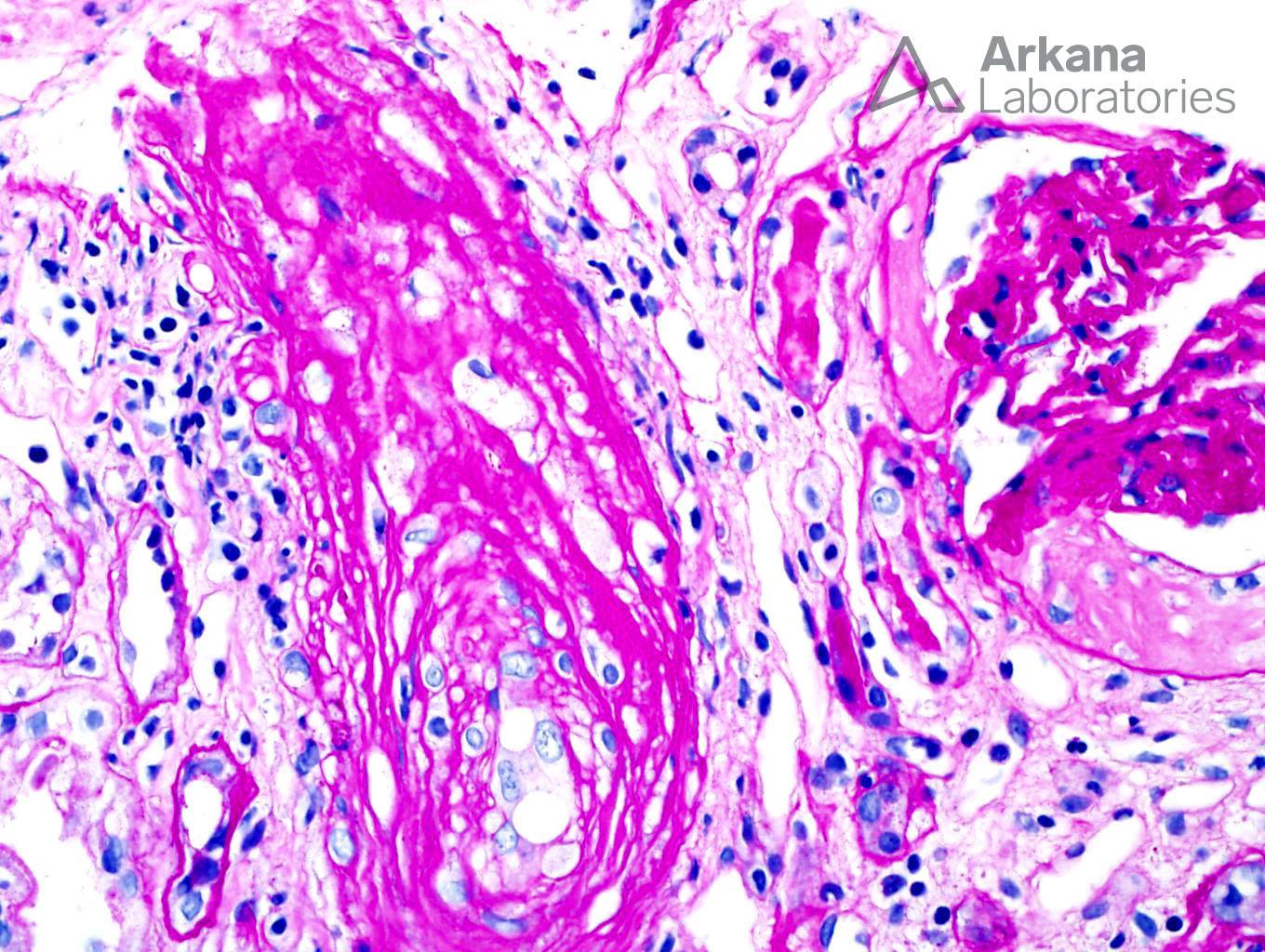
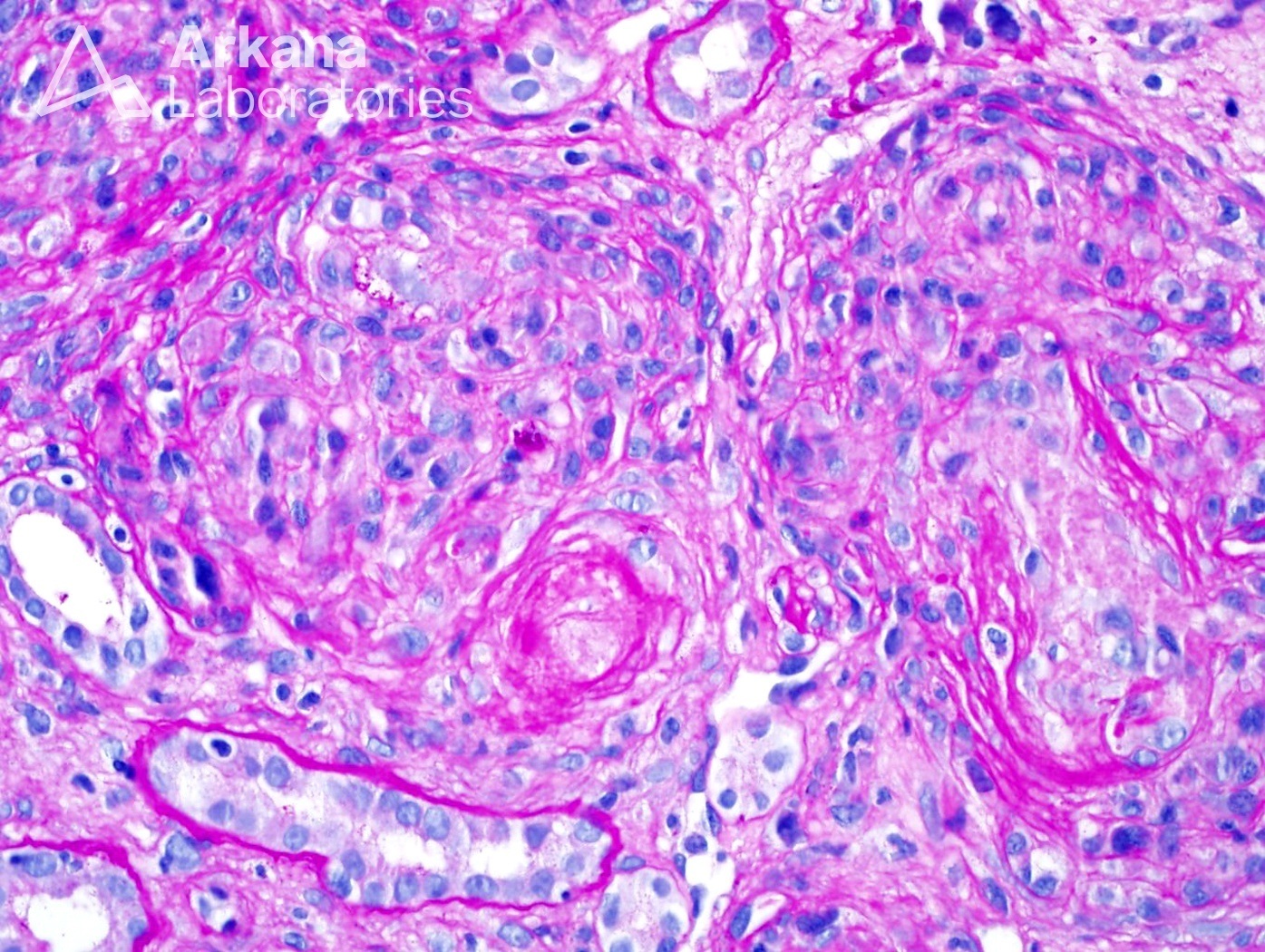
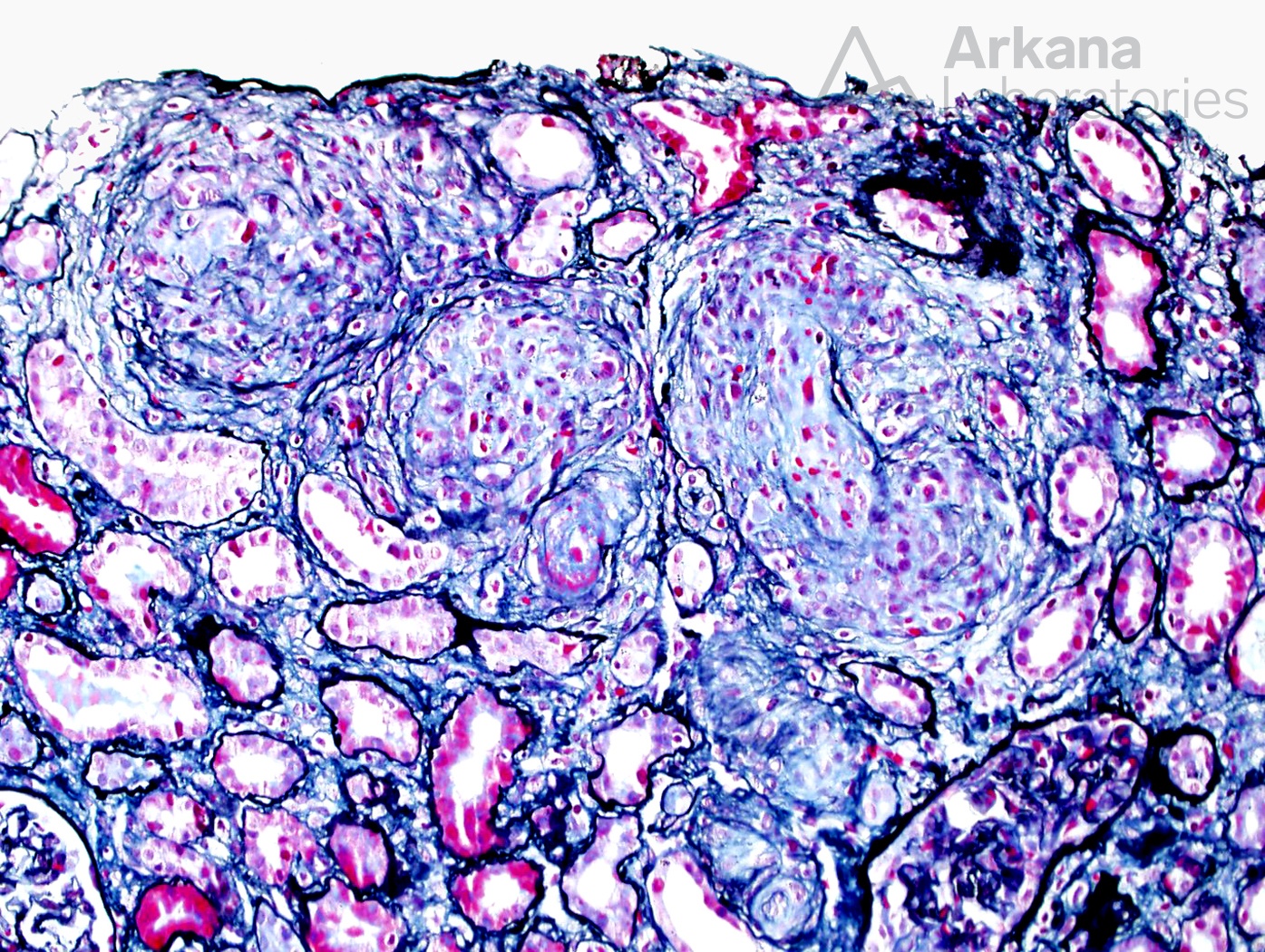
Thrombotic microangiopathy is a pattern that may be seen in a wide spectrum of disease. Histological clues as to origin are few and only moderately associative. For example, arteriolar TMA without glomerular involvement is typical of accelerated hypertension or scleroderma and much less likely to be seen in HUS or TTP. Still, TMA always requires detailed clinical correlation.
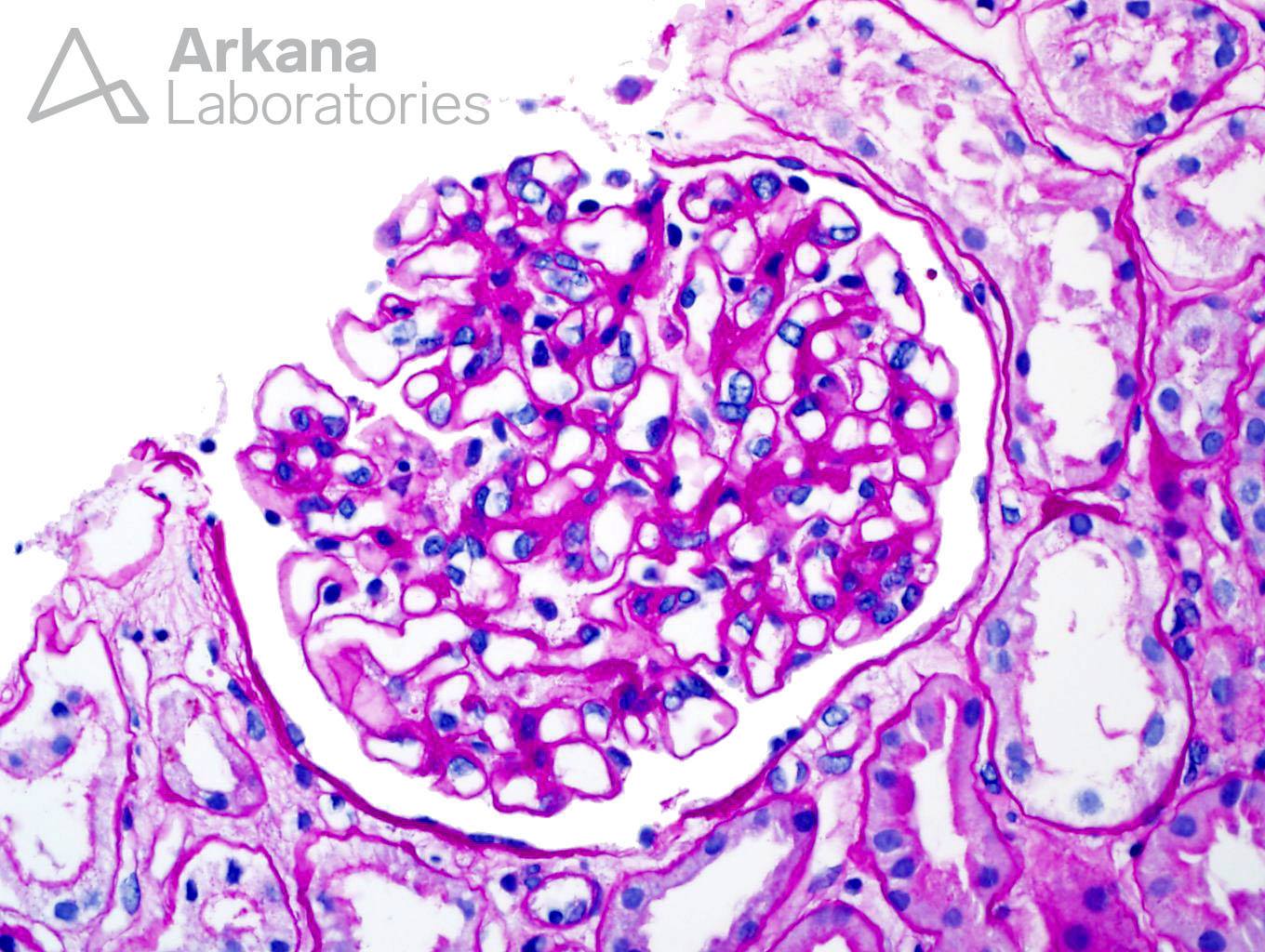
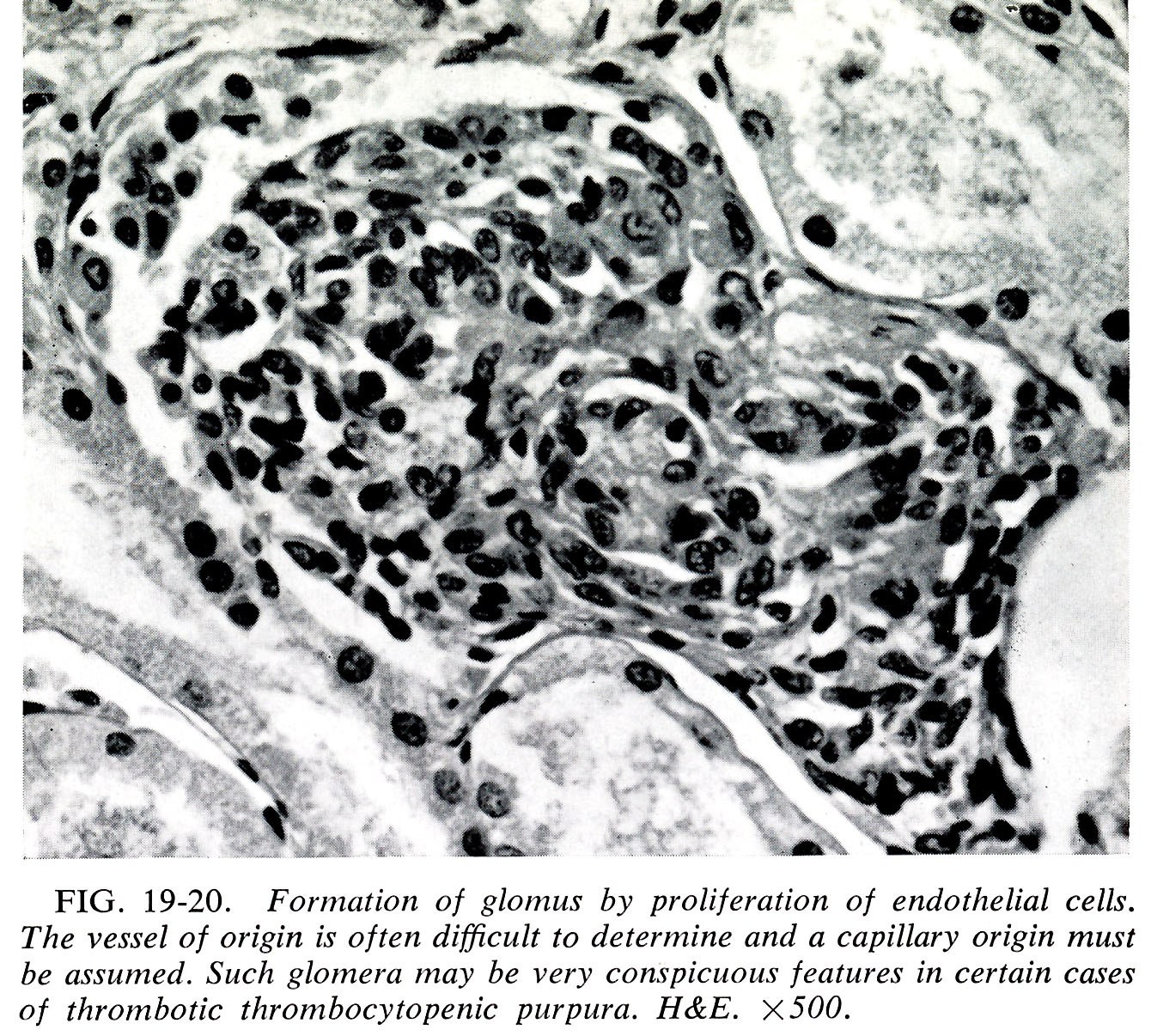
A rather startling feature of the present biopsy is the finding of a “glomeruloid body” composed of a proliferation of endothelial-lined capillaries and arterioles. It is often difficult to determine the capillary origin and as Dr. Robert Heptinstall noted in his First Edition of Pathology of the Kidney (Chapter 19: Pages 564-565, Figure 19-20. 1966) “Such glomera may be very conspicuous features in certain cases of thrombotic thrombocytopenia purpura (TTP).” These features are dramatically illustrated in the paper of MacWhinney et al (1). These “glomera” of cells may sometimes attain the size of glomeruli. They noted that similar proliferations can be seen in radiation nephritis and malignant hypertension, and others have noted them also. This ‘glomeruloid body’ was included in Heptinstall’s subsequent editions (2nd to the 5th Editions) and mentioned but not illustrated in the Sixth Edition. A very similar lesion was produced in an animal model by Dvorak et al (2) by the injection of VEGF which was sufficient for induction of the glomeruloid microvascular proliferations.
These unusual changes appear to be a severe form of microangiopathic change and likely can be seen in association with many, if not all, of the causes of TMA.
References:
1. MacWhinney JB, Packer JT, Miller G and Greendyke RM. Thrombotic thrombocytopenic purpura in childhood. Blood 19 (2): 181-189, 1962
http://tinyurl.com/y7qthtmd
2. Sundberg C, Nagy JA, Brown LF, Feng D, Eckelhoefer IA, Manseau EJ, Dvorak AM, Dvorak HF. Glomeruloid Microvascular Proliferation Follows Adenoviral Vascular Permeability Factor/Vascular Endothelial Growth Factor-164 Gene Delivery. Am J Pathol. 2001 Mar; 158(3): 1145–1160. doi: 10.1016/S0002-9440(10)64062-X
http://tinyurl.com/yazgq5hj
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.