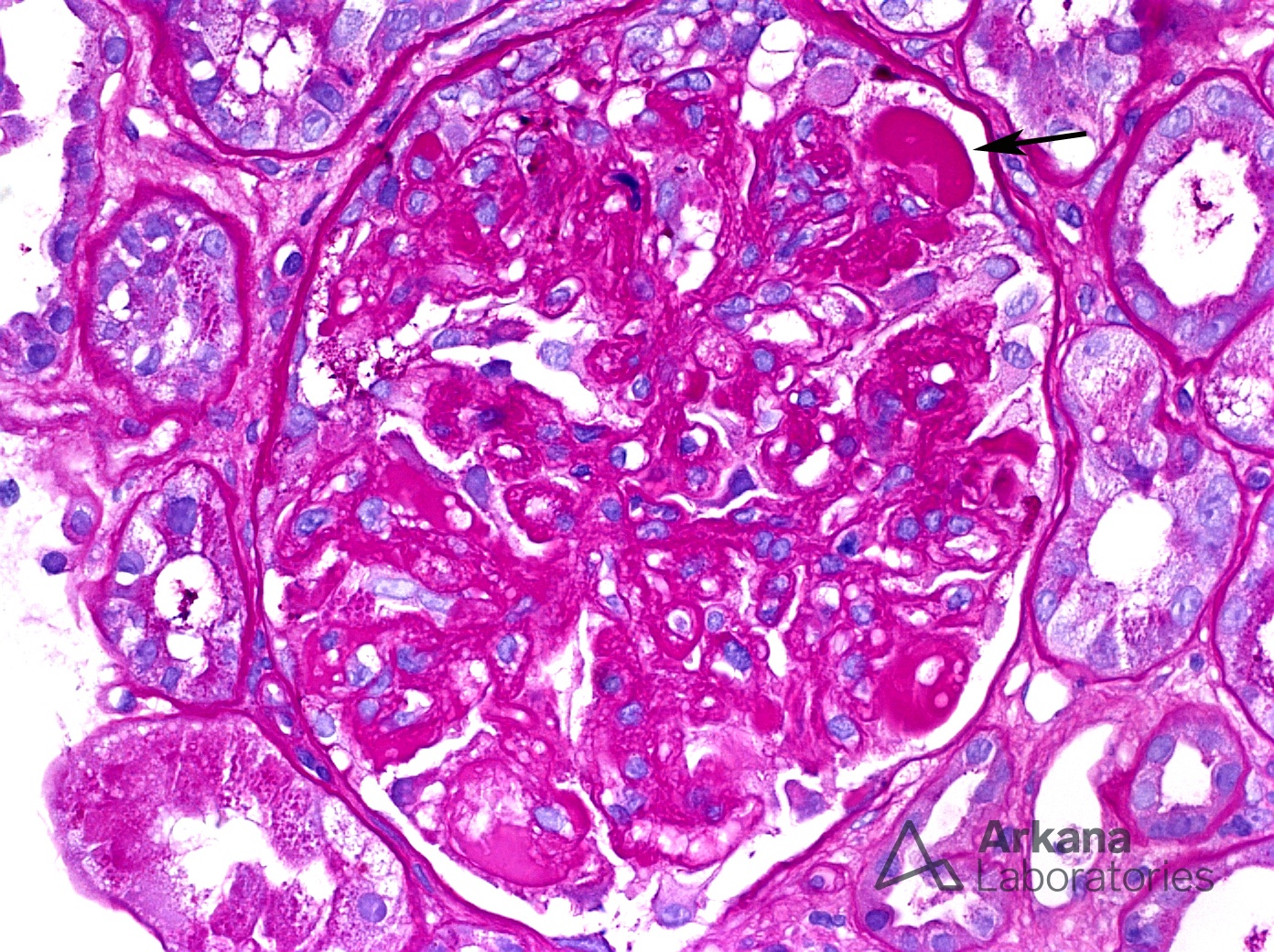
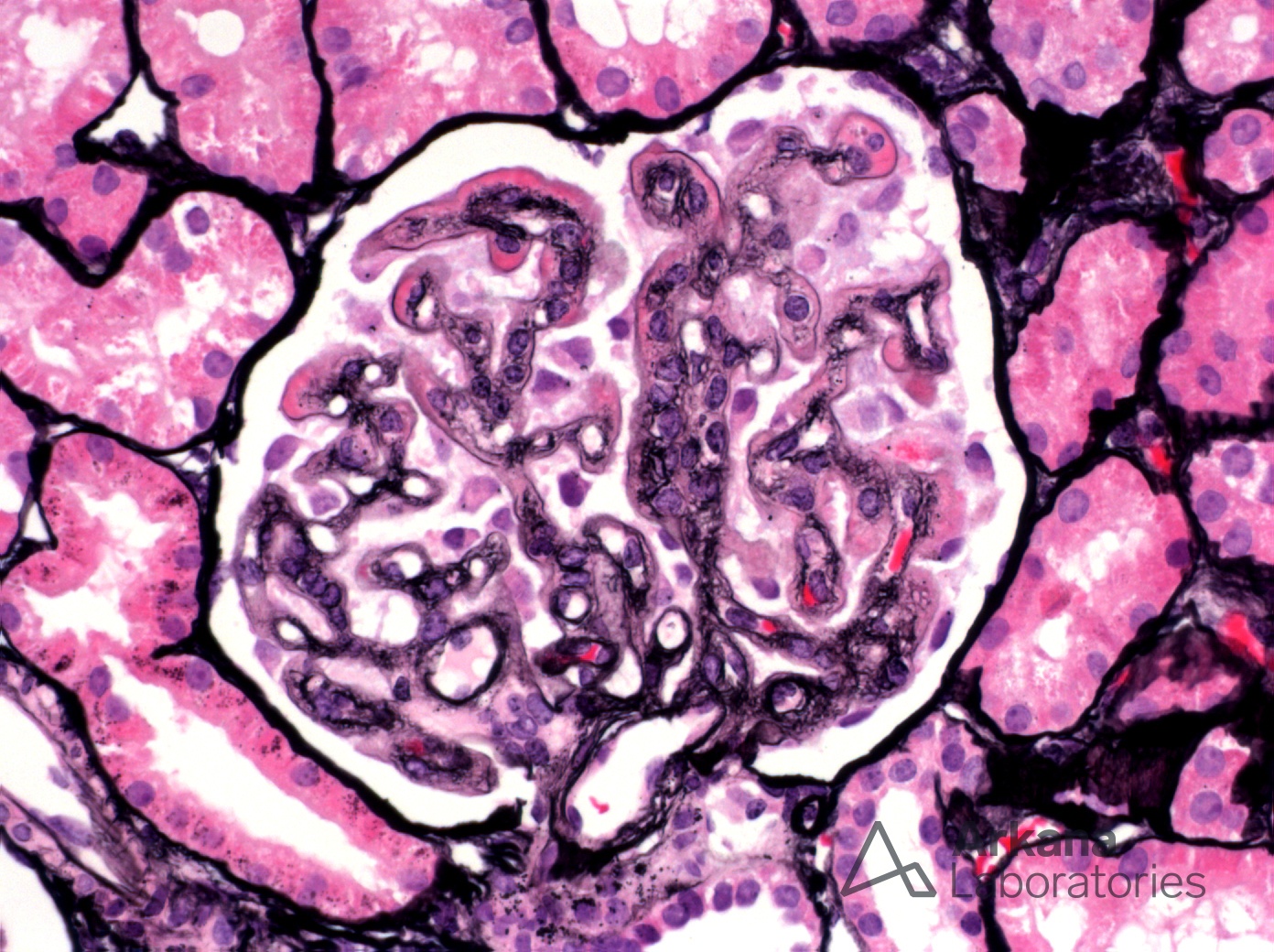
The biopsy shown here is from a seven-year-old female with nephrotic syndrome. Her serum Cr was increased to 0.9 mg/dl and her urine protein/creatinine ratio was 7. She was s/p nephrectomy for renal cell carcinoma and had been treated with bevacizumab for six months prior to the biopsy. Serum C3 and C4 levels were normal and her platelet count was also normal. On biopsy, glomeruli show extensive basement membrane duplication and segmental hyalinosis of the glomerular tuft (arrow). These glomerular changes are characteristic of VEGF inhibitor-associated glomerulopathy. There is evidence to suggest that VEGF production by podocytes is required for maintenance of the adjacent glomerular endothelium fenestrations. As seen in these photomicrographs, pharmacologic disruption of VEGF can result in a glomerular injury. While not pictured here, it is important to be aware that VEGF inhibitor-associated glomerulopathy can also show glomerular staining for IgA and/or IgM but this should not be confused for an immune complex-mediated glomerulonephritis.
Reference:
N Engl J Med 2008; 358:1129-1136
Quick note: This post is to be used for informational purposes only and does not constitute medical or health advice. Each person should consult their own doctor with respect to matters referenced. Arkana Laboratories assumes no liability for actions taken in reliance upon the information contained herein.